Best HCP Engagement Platforms for Pharma in 2026: 12 Compared Across Orchestration, Activation, and Closed-Loop Measurement
.webp)

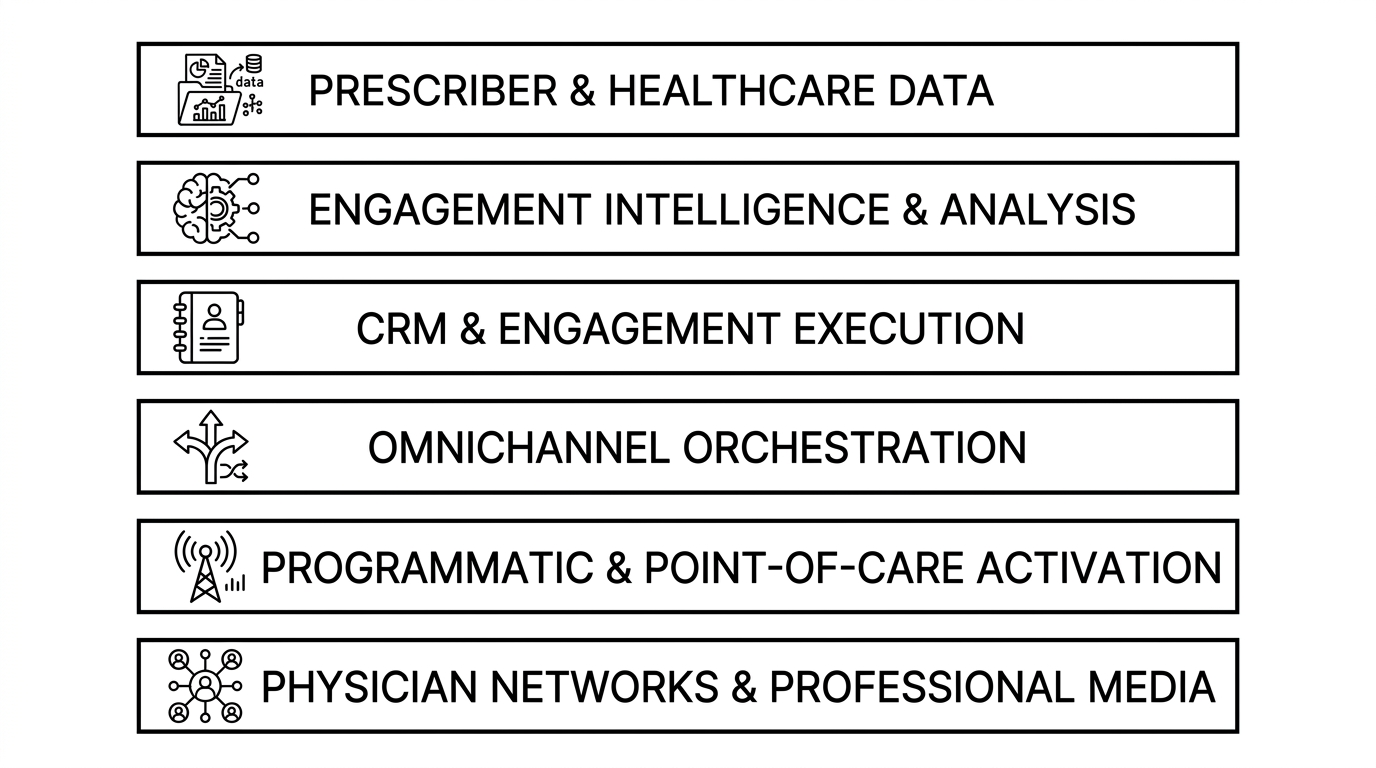
HCP engagement platforms are the software systems pharma commercial teams use to reach healthcare professionals with the right message, through the right channel, at the right moment. The category spans five functional layers: the prescriber-data foundation that establishes who matters, the analysis layer that determines who to engage and why, omnichannel orchestration that sequences next-best-channel and next-best-message across field and digital, programmatic and point-of-care activation that delivers the message, and closed-loop measurement that confirms whether engagement changed prescribing. Unlike static, decile-based outreach that pushes the same cadence to every physician, modern HCP engagement connects prescriber signals, payer access, and real-time behavior to personalize engagement — then measures the result and feeds it back.
No single platform owns the whole stack, and the strongest commercial teams assemble several. Within it, Tellius occupies the intelligence layer: it is the only platform in this comparison that reasons across prescriber, payer, engagement, and unstructured data to determine why an HCP's behavior is shifting, decide the next best move, and re-prioritize from measured outcomes — then delivers a finished engagement plan to the orchestration and activation systems a team already runs.
This guide evaluates 12 platforms across all five layers using eight criteria. It weights one most heavily — a platform's ability to autonomously analyze why HCP behavior is changing and recommend the next move — while noting where teams that prioritize reach, ecosystem fit, or cost will reasonably rank these platforms differently.
Quick reference: which platform for which need
Most enterprise teams use a combination — for example, IQVIA data flowing into a customer-owned warehouse, Veeva for CRM and Crossix for omnichannel measurement, DeepIntent or OptimizeRx for activation, and Tellius reasoning on top to decide who to engage and why.
The functional categories
These categories are complementary, not competitive substitutes — the comparison below covers all six.
The comparison
Veeva ranks first on market presence — the most widely deployed pharma engagement platform, and the system most commercial stacks already run on. Tellius ranks second because it leads the dimension this guide weights most heavily — autonomously analyzing why HCP behavior is shifting and recommending the next move — though it has less market presence than the incumbents. IQVIA and the remaining platforms follow by market presence and capability breadth within their respective layers. Tellius is marked ◐ on orchestration and ✗ on activation reach by design: it decides the engagement, it doesn't execute the send.
How we evaluated
Comparing platforms that sit on five different layers means no single scorecard fits all of them cleanly. A prescriber-data provider and a programmatic ad network do different jobs, and a good one of each looks nothing like the other on paper. The eight criteria below assess each platform on what matters to an omnichannel engagement program: the data that feeds it, the decision about who to engage and why, the last-mile delivery, and the measurement that closes the loop. They map to the columns in the comparison table above.
- Autonomous why + next-move analysis (the single most important differentiator). Whether the platform can, on its own, detect that a healthcare professional's (HCP's) behavior has shifted, diagnose why across every available signal, and recommend the specific next move, without an analyst running the investigation by hand. This guide weights it most heavily, because it is what turns engagement data into an engagement decision.
- Cross-source data reasoning. Whether the platform reasons across prescriber and claims data, payer access, CRM and field activity, digital engagement signals, and unstructured sources like call notes and market research as a single picture, rather than analyzing each in isolation. The reason a behavior changed rarely lives in one source. It lives where they intersect.
- Predictive + agentic AI. Whether the intelligence runs continuously and acts toward a goal (agentic, 24/7) or fires from predefined rules when a person triggers it. Rules-based next-best-action is legitimate and widely deployed; this criterion separates it from autonomous reasoning that re-prioritizes as conditions change.
- Omnichannel orchestration. Whether the platform sequences next-best-channel and next-best-message across field and digital, coordinating rep, email, point-of-care, and programmatic touches into one coherent journey instead of firing each channel independently.
- Activation channel reach. The breadth of channels the platform can actually deliver through: field and CRM, point-of-care at the electronic health record (EHR), programmatic display, and endemic professional media. This is execution, the last mile that puts a message in front of an HCP.
- Closed-loop measurement & attribution. Whether the platform connects engagement back to prescribing behavior and feeds the result into the next cycle's targeting and sequencing, rather than reporting activity metrics that never reconcile to script lift.
- Explainability & governance. Whether outputs are traceable, reproducible, and defensible under pharma compliance review: HIPAA-aligned data handling, audit trails, and logic a medical-legal-regulatory (MLR) reviewer can follow. In 2026 this is increasingly the second buying question after capability fit.
- Works across the existing stack. Whether the platform fits the systems a commercial team already runs (IQVIA or Veeva data, an established CRM, an existing media stack) or requires displacing them. Vendor neutrality matters most for the layers that sit between systems rather than replacing them.
This evaluation weights the first criterion, autonomously analyzing why HCP behavior is changing and recommending the next move, as the primary differentiator. Organizations that weight activation reach, ecosystem fit, deployment speed, or cost most heavily will reasonably rank these platforms differently.
How to choose
Where a team should start depends on which gap is most acute right now: the data foundation, the decision about who to engage and why, the orchestration, or the last-mile delivery. Match the priority to the layer that owns it.
- If your primary need is a prescriber, claims, and reference-data foundation, IQVIA is the foundational data layer. Its prescription, claims, and reference assets underpin most commercial stacks, and nearly every other platform here consumes IQVIA data in some form.
- If your primary need is patient-journey mapping and physician identification, Komodo Health owns this lane. Its encounter-level patient data is built for tracing therapy starts, switches, and the providers along a patient's path.
- If your primary need is understanding why an HCP's behavior is shifting and what to do next, Tellius is built specifically for this. It reasons across prescriber, payer, engagement, and unstructured data to diagnose the change and recommend the next move, then hands a finished engagement plan to the orchestration and activation systems a team already runs.
- If your primary need is pharma CRM and field execution, Veeva is the de facto answer. It is the system of record most commercial stacks already run on, and the hub through which field and omnichannel engagement is planned, logged, and measured.
- If your primary need is agentic, Data Cloud–native engagement on an existing Salesforce footprint, Salesforce Life Sciences Cloud leads here, pairing its Customer Engagement product with Agentforce capabilities for teams standardizing on the Salesforce platform.
- If your primary need is rep next-best-action orchestration, anchor on Aktana / PharmaForceIQ. Its sequencing engine is purpose-built to feed reps the next suggested action inside the CRM, now packaged as an optichannel deployment.
- If your primary need is AI-native omnichannel orchestration, ODAIA is the orchestration specialist, built from the ground up to predict HCP journeys and sequence next-best-channel and next-best-message across field and digital.
- If your primary need is last-mile activation reach, look to DeepIntent for programmatic HCP advertising across display and connected channels, OptimizeRx for point-of-care messaging at the EHR, and Doximity for verified physician-network and professional-media reach.
Key takeaways
Veeva is the most widely deployed engagement platform in pharma commercial. It is the CRM and content system most field and omnichannel teams already run on, now migrating from the wound-down Salesforce partnership to Vault CRM, with Crossix adding omnichannel measurement. Best for pharma CRM, field execution, and closed-loop measurement on a single vendor's system of record.
Tellius is the platform for teams that need to understand why HCP engagement and prescribing behavior is shifting, and what to do next. It is the only platform in this comparison that proactively monitors for those shifts (tracking KPIs continuously across every dimension and surfacing anomalies with their root causes attached), then reasons across prescriber, payer, engagement, and unstructured data to diagnose why the behavior changed, quantify the drivers, recommend the next best move, and re-prioritize from measured outcomes, before shipping a finished engagement plan to the orchestration and activation systems a team already runs. It is used by top-10 and top-20 global pharmaceutical commercial teams; one anonymized top-10 oncology brand reports cutting monthly review prep by 85% and surfacing a $12M underserved-community opportunity (vendor-reported). Where the rest of this comparison shows what an HCP did, Tellius explains why, and delivers the next move before anyone asks.
IQVIA is the reference-data foundation for the industry. Its prescription, claims, and reference assets underpin most commercial stacks, paired with its OCE engagement tools and a growing agentic portfolio (IQVIA.ai and the NVIDIA collaboration). Best for teams that want their prescriber-data foundation and engagement tooling from a single vendor.
Salesforce Life Sciences Cloud is the Data Cloud–native engagement option. Its Customer Engagement product reached general availability in late 2025, with Agentforce agentic features rolling out through 2026. Best for life-sciences teams standardizing on the Salesforce platform that want engagement built on their existing customer-data foundation.
Aktana / PharmaForceIQ is the established rep next-best-action engine. Combined under PharmaForceIQ's January 2026 acquisition and packaged as an "optichannel-in-a-box" deployment, it feeds reps the next suggested action inside the CRM. Best for teams that want proven, CRM-embedded sequencing live in weeks rather than quarters.
ODAIA is the AI-native omnichannel orchestration specialist. Built from the ground up to predict HCP journeys and sequence next-best-channel and next-best-message across field and digital. Best for teams that want modern, journey-based orchestration without the legacy of a rules-era suggestion engine.
DeepIntent is a leading programmatic platform for HCP advertising. A healthcare demand-side platform (DSP) reaching verified providers across display and connected channels, recently expanding into point-of-care inventory at the electronic health record (EHR). Best for digital teams that need compliant, measurable programmatic reach to targeted HCP audiences.
OptimizeRx is a point-of-care messaging leader. It delivers brand and access messages to HCPs inside the clinical workflow at the EHR. Best for teams whose priority is reaching prescribers at the moment of care, close to the prescribing decision.
Doceree is a programmatic network purpose-built for HCP messaging. An identity and advertising platform focused on verified provider targeting across endemic and point-of-care channels. Best for teams that want HCP-specific programmatic delivery with provider-level identity resolution.
PulsePoint is a health-focused programmatic platform. It pairs real-time health signals with DSP delivery across HCP and patient audiences. Best for teams that want data-driven programmatic activation grounded in health-intent signals.
Komodo Health is the patient-journey data specialist. Its encounter-level "Healthcare Map" traces therapy starts, switches, and the providers along a patient's path. Best for teams that need deep patient-journey mapping and physician identification beyond standard prescriber data.
Doximity is the verified physician-network reach platform. It runs the professional network used by the large majority of US physicians, with native and professional-media engagement channels. Best for teams that want to reach verified HCPs through a trusted professional channel.
Who benefits most
Different roles feel the engagement problem from different angles. Here is where the pain concentrates, and what each role is trying to fix.
- Omnichannel engagement lead. Wants field and digital engagement coordinated into one HCP journey instead of a set of disconnected channel campaigns. The pain is that channels and signals live in separate systems, so there is no single read on why an HCP is shifting or which touch to fire next.
- Brand / activation marketer. Wants campaigns that reach the right HCPs at the right moment, and a fast read on what actually moved behavior. The pain is that targeting lists go stale between cycles, and the post-campaign analysis lands too late to change the next flight.
- Commercial operations lead. Owns the rep drop list and the suggestions that flow into the CRM. The pain is reconciling conflicting signals across prescriber data, CRM activity, and media into one prioritized, defensible next action.
- Digital & media manager. Wants efficient, compliant activation across programmatic and point-of-care channels. The pain is proving which engagement actually drove prescribing, rather than reporting impressions and click-through that never reconcile to script lift.
- Field excellence lead. Wants reps focused on the right HCPs with the right message, and a reason behind each suggestion. The pain is that guidance is rules-based and slow to adapt when an HCP's behavior changes mid-cycle.
- Commercial analytics lead. Wants the why behind engagement performance fast enough to act on it. The pain is the multi-day manual investigation cycle that follows every time a number moves and leadership asks what happened.
What separates engagement that knows why from engagement that only knows what
The category has come a long way from list-and-blast. Most teams now run some form of coordinated, multi-channel engagement, and the better programs sequence field and digital touches instead of firing each in isolation. But modern and intelligent are not the same thing. A great deal of modern engagement still runs on a thin definition of intelligence: it knows what happened, and it knows what to send next, but only from rules someone wrote in advance. It does not know why.
The why is the first dividing line. Knowing that an HCP's new-to-brand prescriptions (NBRx) dropped, or that they stopped opening emails, is description. Knowing why is what determines the right next move: a payer moved the brand off tier-2 access, a competitor's medical science liaison (MSL) started visiting, a formulary added a step edit, a switched patient cohort aged out. And the why almost never lives in one place. It sits across prescriber data, payer access, CRM activity, engagement signals, and unstructured sources like call notes and market research. A platform that reads only one of those can describe the change. It cannot explain it.
Adaptation is the second dividing line. Rules-based orchestration fires the same sequence until a person rewrites the rules, and the behavior of HCPs does not wait for that. Engagement that adapts re-prioritizes as conditions change and as measured outcomes come back, a closed loop rather than a one-way pipeline that pushes a plan and waits for the next planning cycle to learn anything. When activation results feed back into the next decision automatically, the program gets sharper every week instead of every quarter.
The third dividing line is what the platform actually hands a person. Lower-maturity tools surface a dashboard or a suggestion and leave the interpretation to the team. Higher-maturity systems hand over a diagnosed answer and a recommended action: the investigation already done, the drivers already quantified, the next move already framed. The difference is the gap between here is the data and here is the decision.
Diagnosing why, adapting continuously from outcomes, and delivering a finished decision rather than a surfaced metric are what separate the top of the engagement-maturity curve from the bottom. They are also a spectrum, not a binary. A platform can be excellent at coordinated activation and still operate on rules rather than reasoning, and that can be exactly the right tool for a given team. The next section lays out that spectrum as four levels.
The HCP engagement maturity model
Engagement programs sit at different points on a spectrum of analytical autonomy. The four levels below describe that spectrum. It is not a ladder where the lower rungs are broken, but a range where each level is the right fit for a particular combination of data maturity, team size, and decision stakes.
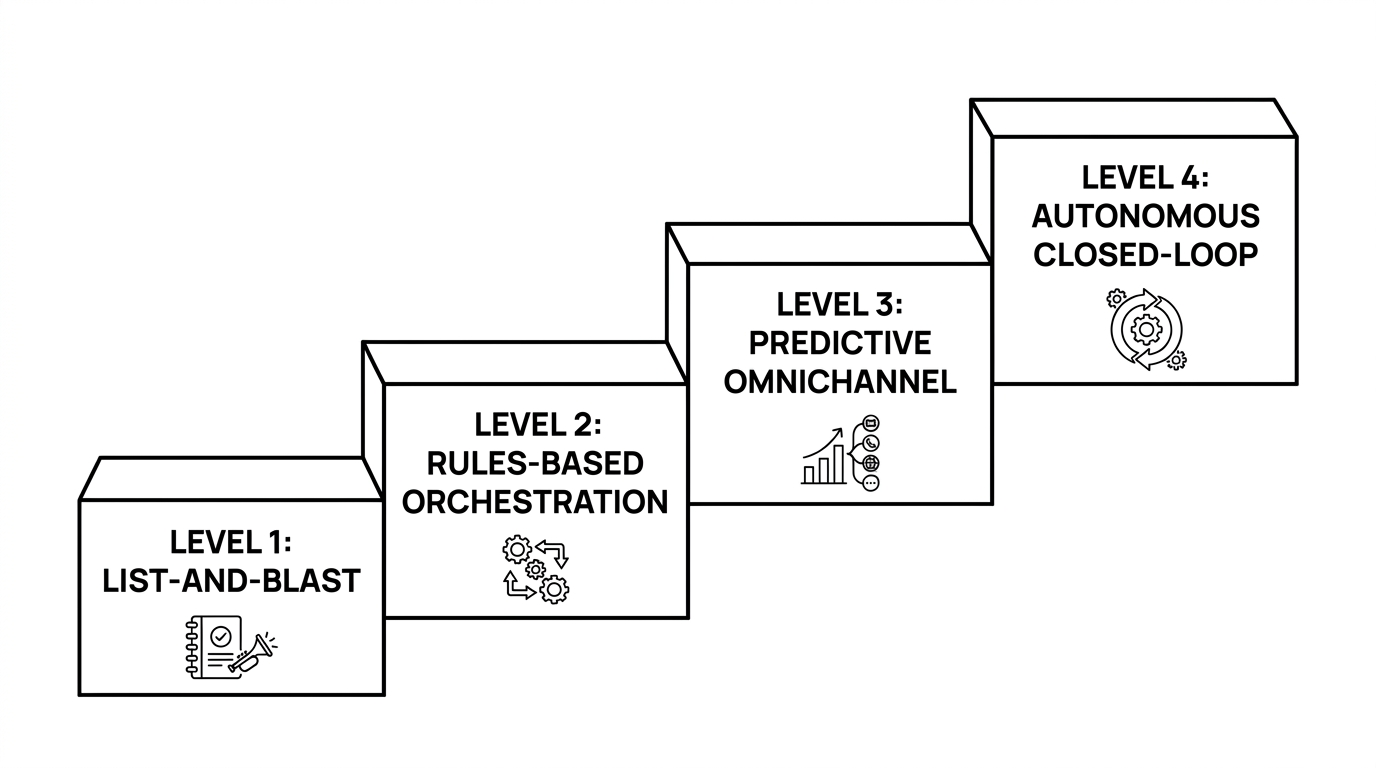
Level 1 — list-and-blast. Static decile lists drive a uniform cadence: the same call plan and the same email rhythm to every HCP in a tier, refreshed annually. This is a legitimate approach for small teams or markets with limited data, where the overhead of orchestration would outweigh the return. Its ceiling is that it cannot react to an individual HCP's behavior between refreshes.
Level 2 — rules-based orchestration. CRM-triggered next-best-action fires from predefined rules. If an HCP attends a webinar, send the follow-up; if a rep logs a call, suppress the email for two weeks. Single channels are optimized in sequence. Widely deployed and genuinely useful, this level coordinates touches well. What it does not do is determine why an HCP's behavior changed, or rewrite its own rules when conditions shift.
Level 3 — predictive omnichannel. Machine-learning propensity models rank next-best-channel and next-best-message across field and digital, refreshed frequently rather than annually. Orchestration specialists such as ODAIA and the PharmaForceIQ/Aktana engine legitimately operate here, and Tellius operates here too. The engagement decision is data-driven and adapts to recent behavior, not only to rules written in advance.
Level 4 — autonomous closed-loop. Agentic reasoning runs continuously: it monitors for shifts across every dimension, diagnoses why a behavior changed across structured and unstructured sources, re-prioritizes from measured outcomes, and ships finished engagement plans without waiting to be asked. Of the platforms in this comparison, Tellius alone operates at this level. The others execute the plan; this is the layer that decides and revises it.
The right level is the one that matches a team's data maturity and decision stakes, not automatically the highest one available.
Platform deep dives
1. Veeva — best for pharma CRM, field execution, and closed-loop measurement on one system of record
Veeva is the most widely deployed commercial platform in pharma. It spans CRM, content and approval management (Vault PromoMats), prescriber and commercial data (OpenData, Compass), and omnichannel measurement via Crossix. After its Salesforce partnership wound down in September 2025, Veeva is migrating customers to its own Vault CRM, a transition that runs toward the end of the decade.
Key capabilities:
- System-of-record CRM for field and omnichannel engagement (Veeva Vault CRM).
- Content and approval management tied to medical-legal-regulatory (MLR) review.
- Prescriber and commercial data via OpenData and Compass.
- Closed-loop measurement via Crossix; Veeva AI Agents (from December 2025) for in-workflow assistance.
Where Veeva excels: It is the system most reps, content, and engagement workflows already run through, which makes it a practical hub for planning, executing, and measuring engagement in one place. Crossix connects engagement to prescribing outcomes within privacy-safe methodology.
Where Veeva falls short: Veeva executes and measures engagement; it does not autonomously reason about why it is changing. Its next-best-action is largely rules- and trigger-based, strong at coordinating the next touch but not at diagnosing across prescriber, payer, and unstructured data why an HCP's behavior shifted in the first place. Its AI Agents are early and assist-oriented rather than built for cross-source root-cause investigation. Because the engagement intelligence is tuned to Veeva's own data, it is also a less neutral analysis layer across a mixed stack.
Pricing: Per-user and per-module enterprise subscriptions across CRM, Vault, and data products, quoted through sales.
Consider if your priority is a single-vendor system of record for execution, content governance, and measurement, and you are prepared for the Vault CRM migration.
2. Tellius — the intelligence layer for HCP engagement
Tellius is Decision AI for the enterprise, the intelligence layer connecting your data to your decisions. In the HCP engagement stack it occupies a narrow, specific role. It is not the data foundation, the CRM, the orchestration engine, or an activation channel. It is the analysis layer that sits between them, reasoning across prescriber, payer, engagement, and unstructured data to decide who to engage, why their behavior is shifting, and what the next move should be, then delivering a finished engagement plan to the systems a commercial team already runs.
How it works in an engagement program. Most platforms in this comparison are built to execute: log the call, send the email, serve the impression, store the record. Tellius is built to decide. Its monitoring layer, Feed, tracks engagement and prescribing KPIs continuously across every dimension (territory, decile, channel, payer, segment) and surfaces anomalies with their root causes attached, rather than waiting for an analyst to notice a dip in a Monday report. When new-to-brand prescriptions (NBRx) slip in a region, or share of business (SOB) erodes among a set of high-decile targets, the system flags it and begins the investigation on its own.
That investigation is where the intelligence layer earns its place. Tellius decomposes the change across sources that normally live in separate tools (IQVIA or Veeva prescriber data, MMIT payer access and formulary status, Veeva CRM call activity, digital engagement signals, and unstructured sources like field call notes and market research transcripts) and reads them as one picture. The why behind an engagement shift rarely sits in a single source. It sits where a tier-2 access loss, a competitor's medical science liaison (MSL) activity, and a drop in rep reach intersect. The reasoning engine quantifies each driver's contribution deterministically, so the same question returns the same answer and a medical-legal-regulatory (MLR) reviewer can trace exactly how it was derived.
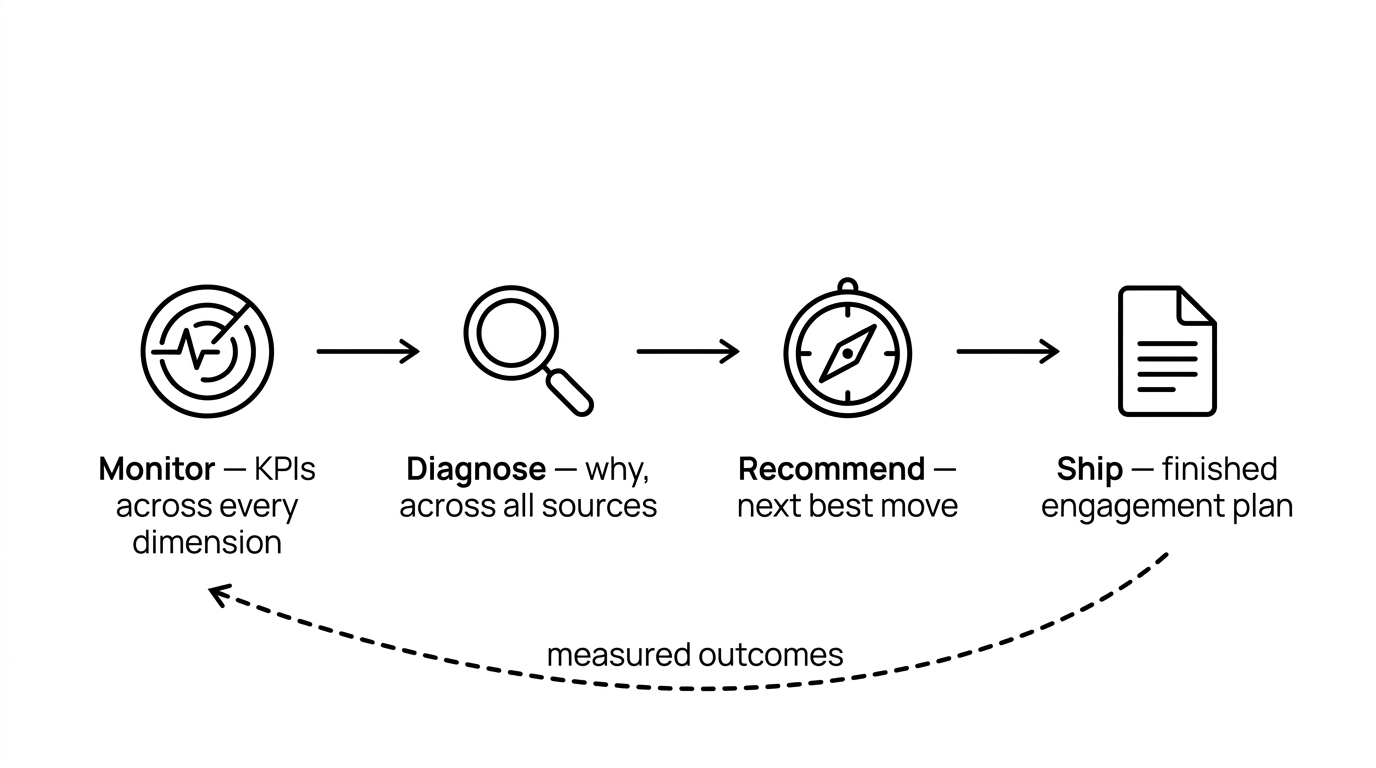
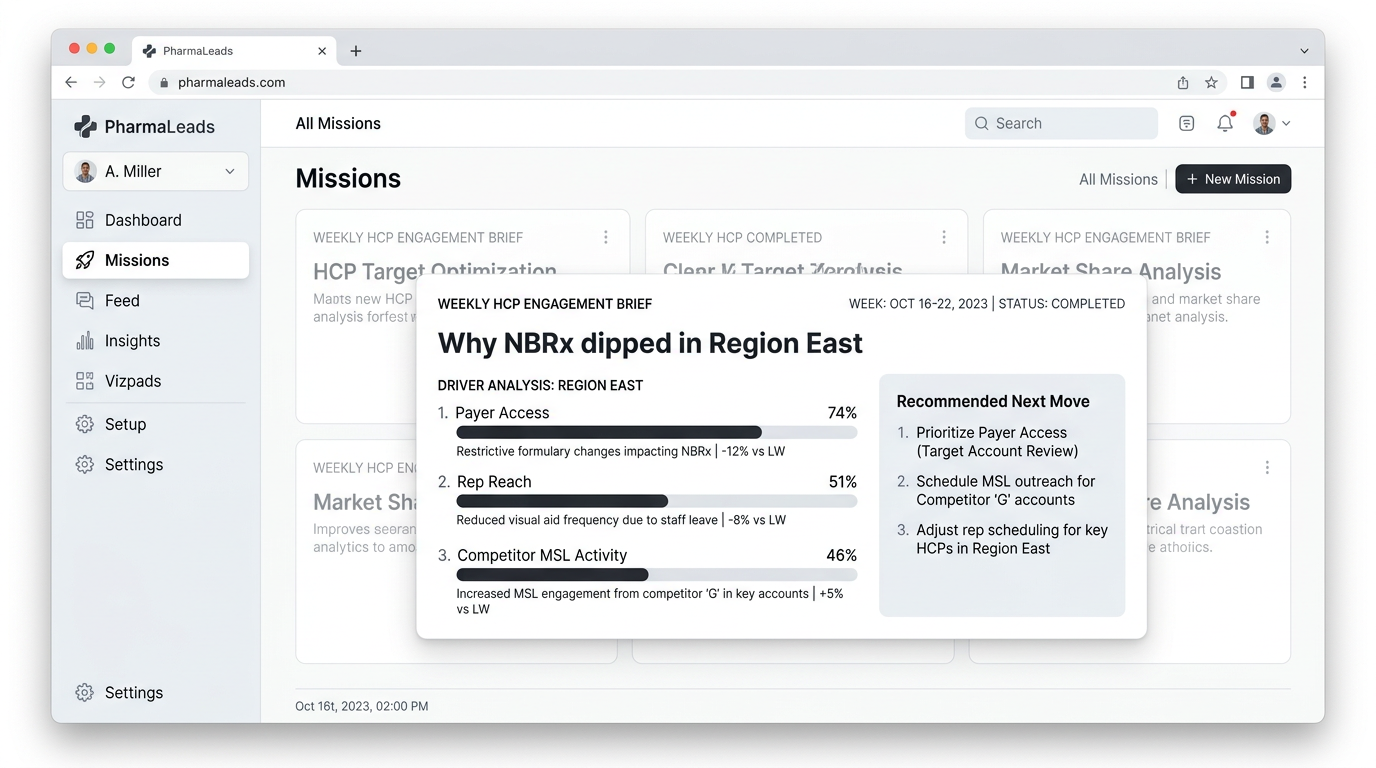
When the answer is ready, Tellius ships it. Through Kaiya, its conversational agent, a brand or omnichannel lead can ask the question in plain English and get the reasoned answer back. Through Kaiya Missions, which are scheduled, multi-step agentic workflows, the same reasoning runs on a cadence without anyone asking: a weekly engagement brief that diagnoses what moved, names the HCPs and territories driving it, and recommends the next sequence, delivered as a finished brief or deck before the Monday call. The recommendation then flows into the orchestration and activation systems the team already runs, and the measured result feeds back into the next cycle's targeting.
Where Tellius excels. It is the only platform in this comparison that automates the full engagement investigation end to end: detecting that an HCP's behavior shifted, diagnosing why across structured and unstructured sources, recommending the next move, and delivering the finished plan before anyone opens a dashboard. Because it reasons over data where it already lives and writes its output into existing systems, it is vendor-neutral by design. It sits on top of IQVIA or Veeva data, an existing CRM, and an established media stack rather than asking a team to replace any of them. And because the reasoning is deterministic and traceable, it clears the governance bar that matters most in pharma: HIPAA-aligned handling, reproducible answers, and an audit trail an MLR reviewer can follow.
Proof points. Tellius is used by top-10 and top-20 global pharmaceutical commercial teams across brand, field, and market-access functions. One anonymized top-10 oncology brand reports cutting monthly review preparation by 85% and surfacing a $12M opportunity in underserved community oncology; a director of commercial data and analytics at a top-20 pharma described getting real-time clarity across commercial and market-access teams (figures vendor-reported, not independently audited).
Where Tellius falls short. Tellius decides the engagement; it does not execute it. There is no media inventory, no field or CRM send mechanism, and no point-of-care network, because the last mile of activation belongs to other platforms. A team whose immediate need is programmatic reach, point-of-care messaging, or rep-facing CRM suggestions will not get that from Tellius alone. The common, intended pattern is to pair Tellius with the orchestration and activation stack a team already owns: Veeva or Salesforce for field and CRM, PharmaForceIQ or ODAIA for sequencing, DeepIntent or OptimizeRx for delivery, with Tellius as the layer that decides what those systems should do next. The narrowness is deliberate. It is what keeps Tellius complementary to the rest of the stack rather than competing with it.
Pricing. Tellius is sold as an enterprise platform on a capacity-based model rather than a self-service per-seat subscription. Pricing scales with data and usage and is quoted through sales.
Best for commercial teams (brand, omnichannel, market access) that need to understand why HCP engagement and prescribing behavior is shifting and what to do next, and that want that analysis delivered as finished work on top of the engagement systems they already run.
3. IQVIA — best for a single-vendor prescriber-data foundation with engagement tooling
IQVIA is the reference-data backbone of pharma commercial, supplying the prescription, claims, and reference assets that most platforms in this comparison consume. It also offers the Orchestrated Customer Engagement (OCE) CRM and an expanding AI portfolio: the NVIDIA collaboration announced January 2025, the IQVIA.ai launch in March 2026, and the Throtle identity acquisition in November 2025. IQVIA has also licensed OCE to Salesforce, a sign of its move toward partnering on execution while it deepens its data and AI position.
Key capabilities:
- Prescription, claims, and anonymized patient-level data (APLD).
- Orchestrated Customer Engagement (OCE) CRM and multichannel tools.
- Reference and master data (HCP/HCO) for targeting and alignment.
- Agentic tooling via IQVIA.ai and the NVIDIA collaboration; identity resolution via Throtle.
Where IQVIA excels: Its data foundation is broad, and most commercial analytics and targeting depend on it, which gives IQVIA a structural advantage when it layers engagement and AI on top. It can connect prescribing, patient-level, and reference data within its own ecosystem.
Where IQVIA falls short: IQVIA's strength is data and breadth, not autonomous diagnosis delivered as finished work. Its tooling is designed to operate within the IQVIA ecosystem, which makes it a less neutral analysis layer for stacks that mix IQVIA data with Veeva CRM and third-party media. The agentic portfolio is real but still maturing toward end-to-end "why did this shift, and what is the next move" investigation across structured and unstructured sources. And the ecosystem-first posture can pull teams toward consolidating on IQVIA rather than reasoning across whatever they already run.
Pricing: Data licensing plus platform and services fees; enterprise contracts quoted through sales.
Consider if your priority is a deep, single-vendor prescriber-data foundation with engagement tooling and AI built on the same data, and you are comfortable standardizing on the IQVIA ecosystem.
4. Salesforce Life Sciences Cloud — best for agentic, Data Cloud–native engagement on a Salesforce footprint
Salesforce Life Sciences Cloud is Salesforce's purpose-built offering for life-sciences commercial and clinical engagement. Its Customer Engagement product reached general availability on October 11, 2025, with more than 70 customers reported at launch, and Agentforce agentic features began rolling out from February 2026. Built on Salesforce Data Cloud, it positions engagement on top of a unified customer-data foundation, and IQVIA's licensing of OCE to Salesforce adds pharma-CRM depth to the story.
Key capabilities:
- Engagement built natively on Salesforce Data Cloud.
- Agentforce agentic assistants rolling out across workflows.
- Unified customer profile across commercial and clinical interactions.
- Platform extensibility, integrations, and inherited compliance and governance.
Where Salesforce Life Sciences Cloud excels: For teams already standardizing on Salesforce, it brings HCP engagement onto the same Data Cloud foundation as the rest of their customer data, which removes a major integration burden. Its Agentforce roadmap is moving quickly toward agentic assistance in engagement workflows, and the IQVIA OCE licensing lends pharma-CRM depth to a young offering.
Where Salesforce Life Sciences Cloud falls short: As a newly GA product, it is earlier in pharma-specific maturity than the incumbents, and its agentic features are still rolling out rather than proven at scale. Its intelligence is oriented toward surfacing and assisting within Salesforce workflows, not autonomous cross-source diagnosis of why behavior changed and what to do next. Activation reach and closed-loop measurement lean on the broader Salesforce and partner ecosystem rather than being native, deep capabilities today.
Pricing: Salesforce platform licensing plus Life Sciences Cloud and Data Cloud consumption, typically tied to existing Salesforce commitments.
Consider if you are standardizing on Salesforce and want Data Cloud–native engagement with a fast-moving agentic roadmap, and you can adopt a newer platform as it matures in pharma.
5. Aktana / PharmaForceIQ — best for proven, CRM-embedded rep next-best-action
Aktana and PharmaForceIQ combined under PharmaForceIQ's acquisition of Aktana in January 2026, pairing Aktana's established suggestion engine with PharmaForceIQ's packaging. The result is marketed as an "optichannel-in-a-box" deployment that feeds reps the next suggested action inside the CRM, with setup reported in weeks rather than quarters.
Key capabilities:
- Rep-facing next-best-action suggestions delivered inside the CRM.
- Sequence and cadence optimization across field and digital touches.
- Pre-packaged optichannel deployment (reported 6–8 week setup).
- Integrations with Veeva and Salesforce CRM environments.
Where Aktana / PharmaForceIQ excels: Its suggestion engine is established and field-proven at feeding reps the next action in their CRM workflow. The post-acquisition packaging shortens what was historically a long orchestration implementation into a matter of weeks.
Where Aktana / PharmaForceIQ falls short: The engine sequences and recommends touches, but it runs on rules and propensity scoring rather than autonomous diagnosis of why an HCP's behavior changed across prescriber, payer, and unstructured data. It tells a rep what to do next; it does not, on its own, investigate the cause behind a shift or deliver a finished explanation. Cross-source reasoning and closed-loop measurement depend on the surrounding stack.
Pricing: Enterprise subscription, typically scoped by brand, geography, and seat count, quoted through sales.
Consider if your priority is getting reliable, CRM-embedded next-best-action live quickly, and the orchestration logic can run on rules and propensity rather than autonomous cross-source reasoning.
6. ODAIA — best for AI-native omnichannel orchestration
ODAIA is an orchestration platform built around predicting HCP journeys and sequencing engagement across field and digital. Its MAPTUAL product applies machine learning to prioritize HCPs and recommend next-best-channel and next-best-message without the legacy of a rules-era suggestion engine.
Key capabilities:
- Predictive HCP journey modeling and prioritization.
- Next-best-channel and next-best-message recommendations across field and digital.
- SaaS deployment with connectors to common CRM and data sources.
- Dashboards for field and marketing teams.
Where ODAIA excels: It is AI-native and purpose-built for omnichannel orchestration, so journey prediction and sequencing are core to the product rather than bolted onto a CRM. For teams that want current orchestration without a legacy rules engine, it is a focused option.
Where ODAIA falls short: ODAIA predicts and sequences engagement, but it is an orchestration specialist rather than an analysis layer that diagnoses why behavior changed across prescriber, payer, and unstructured sources and delivers a finished explanation. Its reasoning is oriented toward the next action, not the root cause behind a shift. Closed-loop measurement and unstructured-source reasoning rely on the wider stack.
Pricing: Enterprise SaaS subscription scoped by brand and user count, quoted through sales.
Consider if your priority is current, journey-based omnichannel orchestration, and root-cause diagnosis across your full data picture sits with another layer.
7. DeepIntent — best for programmatic HCP advertising at scale
DeepIntent is a healthcare demand-side platform (DSP) for programmatic HCP and patient advertising across display and connected channels, with verified provider targeting. In late May 2026 it announced point-of-care integrations with OptimizeRx, epocrates, and Lane4.io, which bring point-of-care delivery into a programmatic buy, with the inventory rolling out from Q3 2026.
Key capabilities:
- Healthcare DSP for programmatic HCP and patient campaigns.
- Verified HCP audience targeting and identity resolution.
- Display, connected TV, and point-of-care inventory (integrations announced May 2026, rolling out from Q3 2026).
- Campaign measurement and outcomes reporting for media.
Where DeepIntent excels: It is a leading programmatic platform for compliant, measurable HCP advertising, with verified provider targeting that media teams rely on. Its 2026 point-of-care integrations (with OptimizeRx, epocrates, and Lane4.io) extend programmatic buying into the EHR, a channel historically bought separately.
Where DeepIntent falls short: DeepIntent delivers and measures media; it is an activation channel, not an analysis layer. It does not reason across prescriber, payer, and unstructured data to diagnose why an HCP's behavior changed or recommend the broader next move. Its scope is the campaign, not the cross-source investigation behind it. Engagement decisions upstream of the media buy come from elsewhere.
Pricing: Programmatic media model, with platform and managed-service fees plus media spend, scoped per campaign.
Consider if your priority is compliant, measurable programmatic reach to targeted HCP audiences, including, now, point-of-care inventory within the same buy.
8. OptimizeRx — best for point-of-care messaging at the EHR
OptimizeRx delivers brand and access messages to HCPs inside the clinical workflow at the electronic health record (EHR), close to the prescribing decision. Its point-of-care network is among the more established in a category that surpassed $1B in spend in 2024, and its inventory is increasingly accessible programmatically.
Key capabilities:
- Point-of-care messaging within EHR and e-prescribing workflows.
- Brand affordability and access messaging at the moment of prescribing.
- HCP reach across a broad EHR network footprint.
- Programmatic availability of point-of-care inventory via DSP integrations.
Where OptimizeRx excels: It reaches prescribers inside the clinical workflow at the point of care, one of the closest channels to the prescribing decision. Its network footprint and the maturing programmatic access to point-of-care inventory make it a focused activation option for that moment.
Where OptimizeRx falls short: OptimizeRx is a delivery channel, not an analysis layer. It does not reason across prescriber, payer, and unstructured data to explain why behavior is shifting or decide the next move beyond the point-of-care message itself. The decision about who to reach and why is made upstream, in another layer.
Pricing: Media and messaging model, with fees tied to program scope and message volume.
Consider if your priority is reaching prescribers at the moment of care inside the EHR, and the upstream targeting and diagnosis live elsewhere in your stack.
9. Doceree — best for identity-based HCP programmatic messaging
Doceree is a programmatic network purpose-built for HCP and patient messaging, centered on provider-level identity resolution across endemic and point-of-care channels. It focuses on verified HCP targeting for programmatic delivery rather than broad audience buys.
Key capabilities:
- HCP-specific programmatic ad network with provider-level identity.
- Endemic and point-of-care channel delivery.
- Verified targeting and frequency management at the provider level.
- Campaign delivery and reporting.
Where Doceree excels: Its provider-level identity resolution is the core of the product, which enables HCP-specific programmatic delivery rather than broad audience targeting. For teams that want identity-grounded programmatic messaging to verified providers, it is a focused option.
Where Doceree falls short: Doceree is an activation network, not an analysis or measurement layer. It does not diagnose why an HCP's behavior changed across prescriber, payer, and unstructured data, and its closed-loop measurement is limited relative to platforms built for attribution. The engagement decision and the read on what worked come from other parts of the stack.
Pricing: Programmatic media model, with platform fees plus media spend, scoped per campaign.
Consider if your priority is identity-grounded programmatic messaging to verified HCPs across endemic and point-of-care channels, with diagnosis and attribution handled elsewhere.
10. PulsePoint — best for health-signal-driven programmatic activation
PulsePoint is a health-focused programmatic platform that pairs real-time health signals with DSP delivery across HCP and patient audiences. Part of the WebMD/Internet Brands family, it emphasizes data-driven targeting grounded in health-intent signals.
Key capabilities:
- Programmatic DSP delivery across HCP and patient (DTC) audiences.
- Real-time health-signal targeting.
- Campaign optimization and measurement for media.
- Access to health-content and intent data.
Where PulsePoint excels: It combines real-time health signals with programmatic delivery, which gives its targeting a health-intent grounding across both HCP and patient audiences. For data-driven programmatic activation in health, it is an established platform.
Where PulsePoint falls short: PulsePoint is an activation and media-optimization platform, not an analysis layer for engagement decisions. It does not reason across prescriber, payer, and unstructured data to explain why an HCP's prescribing behavior changed or recommend the broader next move. Its scope is the media, not the cross-source diagnosis upstream of it.
Pricing: Programmatic media model, with platform and managed-service fees plus media spend.
Consider if your priority is health-signal-driven programmatic activation across HCP and patient audiences, and engagement diagnosis sits in another layer.
11. Komodo Health — best for patient-journey mapping and physician identification
Komodo Health is a patient-journey data specialist built around its encounter-level "Healthcare Map," which traces therapy starts, switches, and the providers along a patient's path. It is used where teams need depth on patient journeys and physician identification beyond standard prescriber data.
Key capabilities:
- Encounter-level patient-journey data (the "Healthcare Map").
- Therapy start, switch, and adherence tracing.
- Physician and care-team identification along the patient path.
- Analytics and software products built on the underlying data.
Where Komodo Health excels: Its encounter-level patient data supports detailed patient-journey mapping and physician identification, which is distinct from prescription-only views. For teams that need to trace switches, starts, and the providers involved, it is a strong data foundation.
Where Komodo Health falls short: Komodo is a data and analytics specialist, not an omnichannel engagement layer. It does not orchestrate or activate engagement, and it is not built to autonomously diagnose why engagement behavior is shifting across prescriber, payer, CRM, and unstructured sources and ship a finished next move. Orchestration and activation belong to other platforms.
Pricing: Data and software licensing; enterprise contracts quoted through sales.
Consider if your priority is deep patient-journey mapping and physician identification beyond prescriber data, with orchestration and activation handled by other parts of the stack.
12. Doximity — best for verified physician-network reach
Doximity operates the professional network used by the large majority of US physicians, offering native and professional-media engagement channels to reach verified HCPs through an environment physicians already use. Its strength is reach to a verified physician audience.
Key capabilities:
- Professional network spanning the large majority of US physicians.
- Native and professional-media engagement formats.
- Verified physician audience for compliant messaging.
- Tools for physician communication and engagement.
Where Doximity excels: It provides reach to a verified physician audience through a professional channel physicians already use and trust. For brand and engagement teams that want presence in that environment, the verified-network reach is its core value.
Where Doximity falls short: Doximity is a reach and media channel, not an analysis, orchestration, or measurement layer. It does not diagnose why HCP behavior is shifting, sequence cross-channel engagement, or close the loop on prescribing outcomes. The targeting decision and the read on impact come from other parts of the stack.
Pricing: Media and engagement model, with fees tied to program and audience scope.
Consider if your priority is reaching verified physicians through a trusted professional channel, with diagnosis, orchestration, and measurement provided elsewhere.
A buyer's checklist: testing the why and the next move
Whichever platforms make your shortlist, the capability hardest to judge from a demo script is whether a platform actually explains why HCP behavior changed and what to do about it, or simply shows that it changed. Most tools demo beautifully on the what. Pressure-test the why with these eight checks.
- Have the vendor demo on a real engagement shift, not a canned dataset: "Show me how this explains why new-to-brand prescriptions (NBRx) dropped among my D1–D3 targets in one region last quarter." If the answer is a dashboard of the drop, you are looking at description, not diagnosis.
- Verify that it reasons across sources in a single investigation: prescriber and claims data, payer access and formulary status, CRM call activity, digital engagement, and unstructured call notes, rather than one source at a time.
- Test whether it runs without being asked: "Does this monitor for shifts continuously and begin the investigation on its own, or does someone have to notice the dip and query it?" A chatbot waiting for input is a different capability than continuous monitoring.
- Probe how it quantifies drivers: can it attribute how much of a shift came from access loss versus reduced rep reach versus competitor activity, with numbers, or does it just list possible factors?
- Look at what it delivers, not only what it surfaces: does it produce a finished recommendation (who to engage, why, and the next move) routed to the right person, or a chart the team still has to interpret?
- Check whether it closes the loop: does the measured outcome of last cycle's engagement feed back into the next recommendation automatically, or is each cycle a fresh manual analysis?
- Confirm the governance story: reproducible answers (same question, same answer), an audit trail, and HIPAA-aligned handling that a medical-legal-regulatory (MLR) reviewer can follow.
- Request named references running in production across brand, field, and market-access teams, not a single pilot.
Bring these eight to every vendor on your shortlist. The answers separate platforms that diagnose from platforms that display.
What about generic tools and DIY?
Before committing to a dedicated platform, it is worth being honest about the cheaper alternatives, because for some teams, at some stages, they are the right call.
General marketing automation (email and campaign platforms) runs cadences and sequences well, and for a small team or an early-stage brand it can be enough to coordinate basic outreach. What it does not do is understand pharma's data or reason about prescribing behavior. It fires on engagement triggers like opens and clicks without connecting to prescriber, payer, or claims data, so it can tell you who opened an email but not why an HCP's prescribing shifted or who to prioritize next. It is built for execution, not engagement intelligence.
General-purpose LLMs (ChatGPT, Claude) are strong at language and at generating a plausible narrative from a data snapshot. Upload a CSV of territory performance, ask why NBRx dropped, and you get a readable hypothesis. That is useful for personal exploration. But there is no persistent connection to your live prescriber, payer, and CRM data, no semantic understanding of what NBRx or share of business means in your business, no audit trail (the same question can return different answers), no HIPAA-aligned handling, and no continuous monitoring. They are personal productivity tools, not governed engagement platforms.
DIY (BI plus spreadsheets plus a capable analyst) can absolutely investigate why an HCP segment shifted, and many teams run exactly this way today. The limits are speed and scale. The investigation is manual and takes days, it runs only when someone asks, and it neither monitors continuously nor ships a finished recommendation on its own. It is a legitimate approach, and it is also the approach a dedicated analysis layer is designed to automate.
Each of these has a real place. The question is whether the job is occasional and exploratory, where they fit, or continuous, governed, and cross-source, where a purpose-built layer earns its cost.
Where HCP engagement is heading: reasoning across the layers
The HCP engagement category is doing two things at once in 2026: consolidating, and going agentic at every layer. The data layer is consolidating. HealthVerity's acquisition of Symphony Health from ICON, completed in mid-May 2026, is the latest move putting more prescriber, claims, and identity assets under fewer roofs. Orchestration is consolidating and packaging. PharmaForceIQ's January 2026 acquisition of Aktana folded a leading suggestion engine into an "optichannel-in-a-box" deployment. CRM is realigning around new owners after the Veeva–Salesforce partnership wound down, with Veeva moving customers to Vault CRM, Salesforce shipping Life Sciences Cloud, and IQVIA licensing its OCE CRM to Salesforce. And activation is going programmatic. Point-of-care media passed $1B in 2024, and by mid-2026 point-of-care inventory was moving into programmatic platforms rather than remaining a separate channel.
Running underneath all of it is the same word: agents. Veeva added AI Agents from December 2025. IQVIA built out IQVIA.ai and an NVIDIA collaboration. Salesforce is rolling out Agentforce. Every layer is racing to put an AI assistant inside its own product.
That race is real, but it mostly solves the wrong problem. The agentic capabilities being added are largely assistive: a copilot that works within one tool's workflow and one tool's data. A CRM agent can draft a rep's follow-up. A media platform's AI can optimize a campaign. A data vendor's model can surface a pattern in its own dataset. None of that reaches the question that actually drives an engagement decision: why is this HCP's behavior shifting, across everything we know about them? That answer does not live inside any single layer. It lives where prescriber data, payer access, CRM activity, digital engagement, and unstructured call notes intersect.
This is why consolidation does not solve it on its own. Putting more data under one roof makes the data more connectable; it does not make it reasoned-over. A team can own every layer and still take days to explain a shift, because the reasoning across layers is still manual.
Over the next two to three years, that is the criterion likely to separate engagement stacks that compound from stacks that merely coordinate. Not whether each layer executes well, and not whether each layer ships an AI assistant, but whether there is a layer that reasons across all of them, diagnoses the why, decides the next move, and learns from the measured outcome. Platforms will increasingly be judged less on the breadth of what they can send and more on the depth of what they can explain. That is the shift this guide is built around.
Tellius vs Veeva
Veeva and Tellius turn up in the same evaluation often, but they operate on different layers of the engagement stack, and many pharma commercial teams run both. Veeva is where engagement is executed and measured: the CRM, the content, the system of record. Tellius is where the engagement decision is made: the analysis layer that reasons across data to decide who to engage and why, then hands the plan to systems like Veeva. The question is not which one to buy. It is which job each one does.
Where Veeva leads. Veeva is the operating system most pharma commercial teams already run on. Its CRM holds the field and omnichannel record, Vault manages content and the medical-legal-regulatory (MLR) approval trail, OpenData and Compass supply prescriber and commercial data, and Crossix provides privacy-safe omnichannel measurement that ties engagement to prescribing outcomes. For executing engagement (planning calls, delivering compliant content, logging activity, measuring reach) Veeva's breadth on one vendor's stack is hard to match, and its Vault CRM migration after the September 2025 wind-down of the Salesforce partnership keeps that execution layer under one roof.
Where Tellius leads. Veeva can tell you what happened and, through rules and triggers, suggest the next touch. What it is not built to do is autonomously diagnose why an HCP's behavior changed across data that lives outside Veeva. When new-to-brand prescriptions (NBRx) slip among a set of high-decile targets, the cause is rarely visible in the CRM alone. It sits at the intersection of prescriber data, a payer's tier-2 access change in MMIT, a competitor's medical science liaison (MSL) activity, a drop in rep reach, and what the reps actually wrote in their call notes. Tellius reasons across all of those at once, quantifies how much each contributed, and ships a finished recommendation (who to re-engage, why, and the next move) before anyone opens a dashboard. Because the reasoning is deterministic and traceable, the same question returns the same answer, and an MLR reviewer can follow exactly how it was derived.
There is a clean division in the data itself. Veeva calls hold the why in narrative form; the warehouse and syndicated feeds hold the what in numbers. Tellius reads them together, the structured Rx trend and the unstructured call note as one investigation, which is precisely the seam a single-vendor CRM is not positioned to cross.
The buyer's question. If your gap is execution (getting reps the right content, logging activity, staying compliant, measuring reach) that is Veeva's job, and Tellius does not replace it. If your gap is the why (explaining fast enough why engagement and prescribing are moving, and deciding the next move across everything you know about an HCP) that is work Veeva's rules-based suggestions were not designed for, and where a dedicated analysis layer earns its place. Most enterprise teams have both gaps.
How they work together. The common pattern is Tellius on top of the Veeva stack. Tellius monitors the full data picture, diagnoses the shift, and decides the next move; that decision flows into Veeva as the plan reps and omnichannel campaigns execute; Crossix measures the result; and the measured outcome feeds back into Tellius's next cycle. Veeva runs the engagement. Tellius decides what the engagement should be. For teams already standardized on Veeva, the analysis layer makes the execution layer's output smarter without displacing any of it.
Tellius vs Aktana / PharmaForceIQ
This is the comparison that sounds like a contradiction. Don't both put a recommendation in front of a commercial team? They do, but they answer different questions, and the difference is the whole point. Aktana / PharmaForceIQ sequences the next touch. Tellius decides what the touch should accomplish and why. Teams frequently run both.
Where Aktana / PharmaForceIQ leads. Aktana's suggestion engine is established and field-proven, and PharmaForceIQ's January 2026 acquisition packaged it into an "optichannel-in-a-box" deployment that goes live in weeks rather than quarters. It feeds reps the next suggested action inside the CRM, optimizes cadence and channel across field and digital, and integrates cleanly with Veeva and Salesforce environments. For getting reliable, rep-facing next-best-action into the field quickly, it is a strong, mature choice.
Where the two differ. Orchestration answers how to deliver engagement: given a goal and a set of rules, what is the best next channel, message, and timing? It is built to optimize the sequence. The intelligence layer answers a question one level up: what should the goal be, and why? Deciding who to engage, and why their behavior is shifting in the first place, requires reasoning across prescriber, payer, CRM, and unstructured data, not optimizing a sequence within predefined rules and propensity scores. On the maturity curve, a modern suggestion engine operates at predictive omnichannel (Level 3); autonomous diagnosis of the why, re-prioritization from measured outcomes, and a shipped recommendation reach the closed-loop level (Level 4).
Put concretely: Aktana / PharmaForceIQ can tell a rep "call Dr. Smith next, with this message, this week." Tellius is built to determine that Dr. Smith's prescribing dropped because a payer moved the brand to step therapy, that twelve similar HCPs in the territory are exposed to the same change, and that the right next move is an access-focused sequence, then to hand that decided plan to the orchestration engine to deliver.
How they work together. The recommendation Tellius decides becomes the input the orchestration engine sequences and delivers. Intelligence decides, orchestration executes, and the measured outcome flows back to the intelligence layer to sharpen the next decision. A team that has already deployed Aktana / PharmaForceIQ does not need to replace it to add diagnostic reasoning. The two stack, with Tellius setting the objective and the orchestration engine carrying it the last mile to the rep. The "isn't this the same thing?" instinct fades once the two questions, what and why versus how, are separated.
Tellius vs ODAIA
ODAIA and Tellius are the hardest pair to tell apart at a glance, because both are AI-native, both are modern, and both produce recommendations. The distinction is the layer each one optimizes for. ODAIA predicts HCP journeys and sequences engagement across channels. Tellius diagnoses why behavior shifted across the full data picture and ships the decision. Some teams could reasonably run both.
Where ODAIA leads. ODAIA is purpose-built and AI-native for omnichannel orchestration. Its MAPTUAL product applies machine learning to predict HCP journeys, prioritize providers, and recommend next-best-channel and next-best-message, without the legacy of a rules-era suggestion engine underneath it. For teams that want current, journey-based orchestration built around prediction rather than static rules, it is a focused, modern option.
Where the two differ. ODAIA's machine learning is oriented toward the next action and the predicted journey. Tellius's reasoning is oriented toward the root cause and the cross-source why, then the finished plan. The difference shows up most clearly on two axes. The first is data scope: an orchestration platform reasons primarily over engagement and prescribing signals, while the intelligence layer also reasons over payer access, claims, and unstructured sources like call notes and market research, because the cause of a shift frequently lives there. The second is output: orchestration optimizes the sequence, while the intelligence layer delivers a diagnosed explanation and a decided next move as finished work, governed and traceable. Both reach predictive omnichannel; only the closed-loop layer adds autonomous diagnosis and learning from measured outcomes.
How they work together. Where both are present, the natural arrangement is the intelligence layer above the orchestration layer. Tellius decides the engagement (who, why, and the next move) and ODAIA sequences and delivers it across field and digital, with results feeding back. ODAIA orchestrates; Tellius reasons. For a team that has invested in modern orchestration and still finds itself spending days explaining why a segment moved, the gap is not in sequencing. It is in the diagnostic layer above it.
Disclosure
This guide is published by Tellius. We are a vendor in this category, and we have positioned ourselves favorably, as every vendor comparison does. We have also worked to make this the most accurate and useful HCP engagement comparison available. Every platform was researched from public sources (analyst material, vendor sites, press releases, and product documentation) and cross-referenced against our competitive research. This evaluation deliberately weights one dimension most heavily: a platform's ability to autonomously analyze why HCP behavior is changing and recommend the next move. That is the dimension Tellius is built for, and it is why Tellius ranks where it does. Teams that weight activation reach, ecosystem fit, deployment speed, or cost most heavily will reasonably rank these platforms differently, and we have tried to give every vendor a genuine recommendation within its specialty. Vendor-reported metrics are noted as such, not as audited benchmarks. If you represent a platform listed here and believe we have mischaracterized it, contact us and we will review and update the relevant section.
See Tellius on your own data
Tellius is the intelligence layer for HCP engagement. It reasons across prescriber, payer, engagement, and unstructured data to tell your commercial team why behavior is shifting and what to do next, then ships the plan to the systems you already run.
Get release updates delivered straight to your inbox.
No spam—we hate it as much as you do!


HCP engagement spans five layers: prescriber data (IQVIA, Komodo Health), engagement intelligence and analysis (Tellius), CRM and execution (Veeva, Salesforce Life Sciences Cloud), orchestration (Aktana/PharmaForceIQ, ODAIA), and activation (DeepIntent, OptimizeRx, Doceree, PulsePoint, Doximity). Most platforms own one layer well; few span more than one.
Evaluate eight dimensions: autonomous why and next-move analysis, cross-source data reasoning, predictive and agentic AI, omnichannel orchestration, activation reach, closed-loop measurement, governance, and stack interoperability. Weight them by your gap. The hardest to judge from a demo is whether a platform explains why behavior changed, not just that it did.
Targeting decides who to prioritize (prescriber scoring, deciles); engagement decides how and when to reach them, and why their behavior is shifting. They are adjacent. This guide covers engagement, orchestration, and activation; for prescriber scoring and targeting platforms, see the HCP targeting guide.
Veeva (AI Agents), IQVIA (IQVIA.ai), Salesforce (Agentforce), and Tellius all describe agentic capabilities, but most are assistive copilots working inside one tool's workflow and data. Autonomous, cross-source reasoning that runs continuously and ships a finished recommendation is rarer, and the dimension this guide weights most heavily.
Explaining why requires reasoning across prescriber, payer, CRM, and unstructured data in one investigation, not describing what changed in one source. Tellius is built specifically for that cross-source diagnosis; data and CRM platforms surface the what; orchestration tools recommend the next touch without diagnosing the cause.
Veeva (via Crossix) and IQVIA offer genuine closed-loop measurement tying engagement to prescribing outcomes; activation platforms report campaign-level outcomes. Tellius closes the loop differently, feeding measured outcomes back into the next engagement decision automatically rather than reporting them as a standalone metric.
Compare on reproducibility, audit trail, and HIPAA-aligned handling. CRM and data incumbents (Veeva, IQVIA, Salesforce) inherit mature governance. For the analysis layer, check whether answers are deterministic and traceable for medical-legal-regulatory (MLR) review. Tellius's reasoning engine is built to return the same answer and show its derivation.
It depends on your primary need. For CRM and field execution, Veeva. For a prescriber-data foundation, IQVIA. For programmatic activation, DeepIntent or OptimizeRx. For understanding why HCP behavior is shifting and the next move, Tellius. For AI-native orchestration, ODAIA. Most enterprise teams combine several.
Tellius is the analysis layer; Veeva is the execution layer. Tellius diagnoses why HCP behavior shifted across prescriber, payer, CRM, and unstructured data and decides the next move; Veeva runs the CRM, content, and measurement that execute it. They are complementary, and Tellius commonly sits on top of the Veeva stack.
Tellius reasons across whatever data a team already runs, including IQVIA data, to diagnose why behavior changed and recommend the next move. IQVIA is the prescriber-data foundation, plus engagement tooling, that many of those signals originate from. Tellius is vendor-neutral analysis on top; IQVIA is the data beneath.
Tellius decides what the engagement should accomplish and why; Aktana / PharmaForceIQ sequences how to deliver it. The orchestration engine optimizes the next touch from rules and propensity scoring; Tellius autonomously diagnoses the cause of a shift across sources and ships the decision the orchestration engine then executes.
Tellius and ODAIA are both AI-native but sit on different layers. Tellius diagnoses why behavior shifted across prescriber, payer, and unstructured data and delivers a finished decision; ODAIA predicts HCP journeys and sequences next-best-channel and next-best-message. The intelligence layer commonly sits above the orchestration layer.
Veeva is the incumbent system of record with the broadest pharma footprint, now migrating to Vault CRM. Salesforce Life Sciences Cloud is newer (GA October 2025), Data Cloud–native, with a fast Agentforce roadmap, strongest for teams already standardizing on Salesforce. The choice usually follows your existing platform commitment.
Aktana / PharmaForceIQ and ODAIA are the orchestration specialists; Veeva and Salesforce include rules-based suggestions. For how next-best-action fits a broader strategy, see the AI for Next Best Action guide. Orchestration executes the sequence; deciding the action and why is a separate, upstream layer.
No platform owns all five layers well. Veeva and IQVIA span the most (data, execution, and measurement) but neither is built for autonomous cross-source diagnosis, and neither owns programmatic activation reach. The strongest commercial teams assemble several platforms across layers.
It varies by layer. Packaged orchestration (PharmaForceIQ's optichannel-in-a-box) reports a 6–8 week setup; CRM migrations such as Veeva Vault run far longer, multi-year for large organizations. An analysis layer that sits on existing data avoids displacing systems, though enterprise data integration still requires a partnership phase.
Pricing models differ by layer. CRM and data platforms use per-user or per-module subscriptions and data licensing; activation platforms use media-spend models; analysis platforms such as Tellius use enterprise capacity-based pricing. Few publish list prices, and most are quoted through sales and scale with data, seats, or spend.
No. A vendor-neutral analysis layer reasons over data where it already lives and writes its output into existing systems, so it sits on top of an existing Veeva or Salesforce CRM, IQVIA data, and a media stack rather than replacing them. Activation execution stays where it is.
Interoperability varies. Data and CRM incumbents tend toward their own ecosystems (IQVIA, Veeva), which is efficient if you standardize on them. Activation DSPs such as DeepIntent and a vendor-neutral analysis layer such as Tellius are designed to work across whatever data and systems a team already runs.
Demo it on a real shift: ask it to explain why NBRx dropped in a region last quarter. If it shows the drop on a dashboard, that is description. If it decomposes the cause across sources with quantified drivers and a recommended next move, that is diagnosis. The buyer's checklist above operationalizes this.
.webp)
Best Pharma Market Access Analytics Platforms in 2026
This blog compares the best pharma market access analytics platforms in 2026, evaluating how each solution helps teams navigate complex payer dynamics, pricing strategies, and access barriers. It highlights a key shift in the market: traditional BI tools struggle with fragmented, slow-moving data, while modern platforms combine real-time data integration, semantic understanding, and AI-driven automation. The guide outlines what to look for—such as multi-source data federation, explainable insights, and automated root cause analysis—and shows how leading solutions enable faster detection of payer changes, improved pull-through, and more proactive, data-driven market access decisions.
.png)
Best AI Platforms for Pharma Field Force Effectiveness and Sales Analytics in 2026: 10 Platforms Compared (Plus 3 General BI Alternatives)
A 2026 comparison of 10 AI platforms for pharma Field Force Effectiveness, focused on what actually separates “agentic” FFE analytics from dashboards: automated deep insights (root cause), proactive monitoring, governed Q&A, pharma data integrations, and workflow orchestration—plus clear “best for” recommendations by use case and team maturity.
.webp)
Best AI Platforms for Pharma Commercial Analytics in 2026: 11 Platforms Compared
This guide compares the 11 best AI platforms for pharma commercial analytics in 2026, evaluating how each supports brand performance, market access, patient analytics, field force effectiveness, incentive compensation, and omnichannel engagement. It highlights a key shift in the market: traditional BI and SFE tools focus on reporting what happened, while newer AI platforms differentiate by investigating why performance changed. The post breaks down core capabilities like root cause analysis, data integration, governance, and agentic workflows—helping pharma teams identify which platforms can deliver faster, more actionable insights across commercial operations.