The Best HCP Targeting Platforms for Pharma: A Guide to AI-Powered Prescriber Intelligence
.jpg)

AI-powered HCP targeting is a pharmaceutical commercial approach that uses machine learning to identify, score, and prioritize healthcare professionals most likely to prescribe or increase prescribing. Unlike traditional decile-based targeting that ranks HCPs by historical prescription volume alone, AI-powered platforms combine prescription data (IQVIA, Symphony), CRM activity (Veeva, Salesforce), digital engagement, claims data, and payer access to predict future potential and physician responsiveness. For commercial teams, this means building unified prescriber intelligence—finding "rising star" HCPs 60-90 days before competitors, detecting prescriber disengagement early, and adjusting targets weekly instead of annually. Tellius is an AI-powered HCP targeting platform purpose-built for pharma—combining unified prescriber intelligence with agentic analytics that continuously monitors, scores, and alerts on which HCPs deserve attention this week.
Your HCP target list was finalized 8 months ago. Since then, 400 physicians in your territories changed their prescribing behavior—some started writing more, some switched to competitors, some stopped seeing reps entirely. Your decile rankings can't tell you which is which. And by the time the next annual refresh arrives, you've spent thousands of calls on HCPs unlikely to move.
This is the fundamental problem with traditional HCP targeting: stale data, incomplete profiles, and no connection to what actually drives prescribing decisions.
AI-powered HCP targeting changes the equation. Instead of static decile rankings based on last year's scripts, leading pharma commercial teams deploy platforms that build unified prescriber intelligence—combining prescription data, CRM activity, engagement signals, payer access, and competitive dynamics to score HCPs on future potential, not past volume, and update targets weekly instead of annually.
Key Findings:
- AI-powered HCP targeting identifies high-potential physicians 60-90 days before competitors using unified prescriber intelligence
- Static decile rankings miss HCPs with high untapped potential—favorable access, right patient mix, low current share
- Purpose-built platforms deploy in 8-12 weeks; custom builds take 6-12 months
- One biotech saw 30% increase in starts within six months using ML-based targeting
- Continuous agentic monitoring detects prescriber churn before quarterly reviews surface it
Why Your CRM Knows Almost Nothing About Your HCPs
Open your CRM right now. Look at any HCP record. What do you actually have?
Most pharma organizations find the same sparse profile: master data (address, specialty, NPI—often with duplicates), basic segmentation (A/B/C/D or a decile from last year), date of last sales visit (if logged), and maybe newsletter subscription status.
That's it. You can't personalize engagement when all you know is "Dr. Smith is a D7. Last visit was March."
Compare this to consumer industries. Amazon knows your purchase history, browsing behavior, and click patterns. Booking.com shows reviews, amenities, guest feedback, and aggregated ratings across dozens of dimensions. These platforms have built "vertical search"—purpose-built intelligence engines matching criteria to comprehensive profiles.
Pharma CRM? "Dr. Smith is a D7. Last visit was March."
This information gap creates real commercial consequences. Reps walk into calls blind. Territory reviews compare activity metrics rather than outcomes. High-potential HCPs hide below decile thresholds because they weren't writing enough last year—even though their patient mix, payer access, and engagement patterns suggest enormous untapped potential. Prescriber churn goes undetected for 90+ days because static lists can't flag declining engagement until the quarterly review.
According to McKinsey's research on pharma commercial analytics, companies scaling advanced analytics for commercial operations see 15-30% improvements in EBITDA over five years. But you can't get there with CRM data capturing a fraction of available HCP intelligence.
What HCP Targeting Actually Needs to Accomplish
Most HCP targeting conversations start with features: "Our platform has predictive scoring." "We do lookalike modeling." "We detect churn." But commercial leaders don't buy features. They buy solutions to problems they face every week.
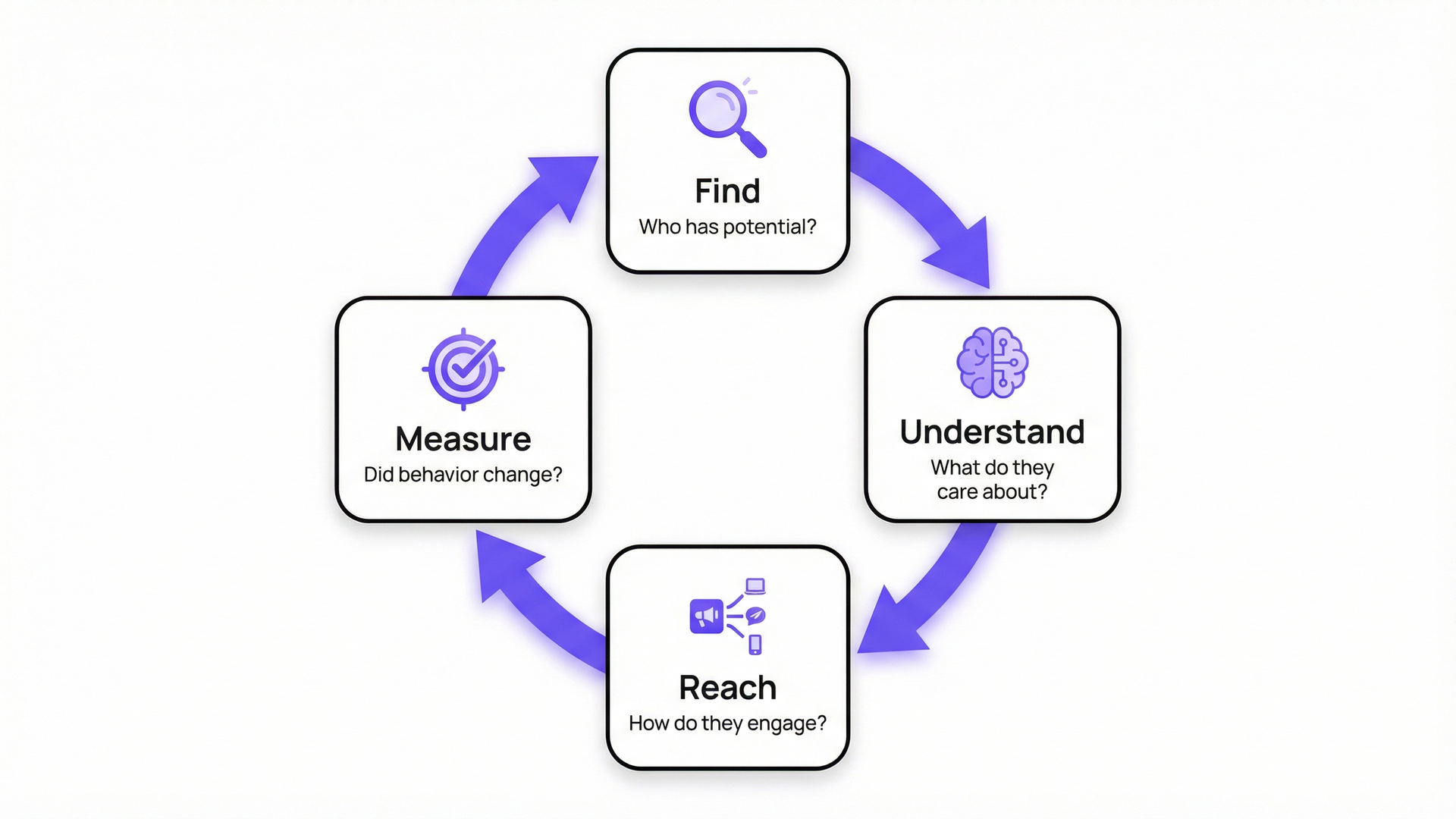
Here are the four things that actually matter—and why static decile rankings fail at all of them.
Finding the Right HCPs (Beyond Volume)
Deciles rank by historical volume. But volume doesn't equal potential.
Consider two endocrinologists in the same territory. Dr. A writes 100 scripts per month—a D1, top of every target list. Dr. B writes 30 scripts—a D4, barely worth a visit. But look deeper: Dr. A has 105 eligible patients and 95% penetration. She's maxed out. Dr. B has 200 eligible patients and 15% penetration. Her payer mix just improved when a major plan added your brand to formulary. She's been detailed twice.
Which physician represents more opportunity?
Deloitte's research on pharma commercial transformation confirms leading companies are shifting from volume-based to potential-based targeting, using AI to create 360-degree views integrating internal and external data. AI-powered targeting surfaces HCPs with high untapped potential: favorable payer mix, right patient population, demonstrated category interest, and low share of business despite high category activity.
Understanding What Each HCP Cares About
Not all HCPs respond to the same message. Some care about efficacy data—clinical trial results and head-to-head comparisons. Others focus on patient outcomes—real-world evidence and satisfaction data. Others prioritize access—they won't prescribe if patients face prior authorization hurdles or high out-of-pocket costs.
HCPs reveal priorities through behavior: publications they author, congresses they attend, digital content they engage with, questions during rep visits, and public communications on LinkedIn and practice websites.
As one commercial analytics director put it: "Would you book a hotel without reading reviews? Then why engage an HCP without knowing what they're talking about?"
PwC's research on AI-powered personalization in pharma reinforces this: with access to HCPs increasingly constrained and competition for their attention intensifying, companies that can deliver personalized, compliant content gain measurable advantage—but only if the targeting data feeding those systems reflects actual HCP preferences, not stale segmentation.
Reaching HCPs Through the Right Channel
"Omnichannel" has become meaningless—a buzzword meaning "we send emails and also have reps." The real question: Is this HCP digitally savvy? What does their behavior tell you about engagement preferences?
An HCP publishing only in peer-reviewed journals probably isn't checking LinkedIn. An HCP with video consultations, active LinkedIn presence, and digital event participation should be offered digital communication options.
According to BCG's analysis of pharma commercial models, the most effective strategies match channel to physician preference rather than applying uniform playbooks. Indegene's 2024 HCP Digital Affinity Report takes this further, categorizing physicians into digital enthusiasts, regulars, explorers, and novices—and finding that digital affinity doesn't simply correlate with age. You don't define the channel—you identify where each HCP actually engages.
Measuring Impact (Not Just Activity)
Traditional metrics—calls made, reach percentage, frequency targets—don't prove anything moved. A rep can hit 100% call plan attainment while NBRx declines. Activity isn't impact.
Impact measurement requires comparing outcomes. Did HCPs receiving AI-prioritized engagement prescribe more than similar HCPs who didn't? Did territories using AI targeting outperform traditional approaches? Can you attribute prescription changes to specific targeting decisions?
McKinsey's work on pharma commercial spend optimization found that for the same brand, promotion responsiveness for HCPs whose patients have disadvantaged managed-care access can be as low as one-fifth the impact per detail compared with HCPs at parity access—making access-adjusted targeting essential to measuring real commercial impact.
From Static HCP Lists to Dynamic Prescriber Intelligence
The shift from traditional to AI-powered HCP targeting isn't incremental improvement. It's structural change in how commercial teams build and maintain unified prescriber intelligence.
What makes AI targeting work? Three capabilities operating together to create unified prescriber intelligence.
McKinsey's research on digital transformation in pharma found that most pharmaceutical firms remain stalled at the experimentation stage, treating AI pilots as one-off initiatives rather than building repeatable commercial engines. The companies making real progress invest at least 20% of EBITDA on digital and analytics programs. The three capabilities below are what separate pilot-stage targeting from operational unified prescriber intelligence.
Unified HCP Intelligence
AI targeting starts with data unification. Pre-built connectors to IQVIA, Symphony, Veeva, Salesforce, and payer databases pull prescribing patterns, field activity, engagement signals, and access reality into a single HCP profile. But connection isn't enough—the platform must resolve HCP identities across sources. When IQVIA shows Dr. Smith at one address and Veeva shows "Smith, J." at another, the system recognizes these as the same physician with a unified timeline.
Patient-level data (APLD) adds another dimension: true patient mix visibility. You see not just that an HCP writes in your category, but what kinds of patients they treat, how they're covered, and whether the population matches your brand's profile.
Predictive Scoring with Explainability
Machine learning models trained on HCPs who increased prescribing reveal patterns predicting future growth. What characteristics did "rising star" physicians share before they started writing more?
Lookalike modeling extends this: "Find 500 HCPs who look like our best converters but aren't on anyone's radar." These are the physicians static targeting misses because they fall below historical volume thresholds.
Critically, scores must be explainable. Black-box rankings erode field trust. When a rep asks "Why is this HCP flagged?" the platform should show drivers: recent payer access improvement, declining competitor share, increased digital engagement, patient mix alignment.
Continuous Monitoring and Action
Static target lists decay from the moment they're published. AI agents watching HCP behavior continuously solve this problem.
When a high-value target stops responding—calls declined, email engagement dropped—the system alerts before quarterly reviews surface the churn. When a payer adds restrictions, scores adjust automatically. When a competitor gains ground, the platform flags affected physicians and recommends response.
This is what Gartner calls "agentic AI"—systems that take initiative, monitor continuously, and act on behalf of users. For HCP targeting: pre-call briefs generated automatically, weekly priority lists pushed to reps, and proactive alerts when targeting assumptions no longer hold. (For more on how agentic analytics applies to pharma commercial operations, see Tellius AI Agents.)

Data Sources That Power HCP Targeting Platforms
Effective HCP targeting requires unifying data most organizations keep in separate systems.
Prescription and Claims Data
IQVIA (Xponent, DDD, PlanTrak), Symphony Health, and Komodo Health provide the foundation: who's prescribing what, in what volumes, how that's changing. IQVIA's own research on AI-powered targeting confirms that multi-source algorithms—combining patient base, professional associations, and prior prescribing behavior—outperform single-dimension volume targeting. APLD adds patient mix visibility—what kinds of patients they treat and how those patients are covered.
CRM and Field Activity
Veeva CRM and Salesforce Health Cloud capture field activity: calls made, samples dropped, speaker program attendance, and conversation substance. This reveals which HCPs are engaged, which are declining meetings, and where execution gaps exist.
Payer and Access Data
MMIT, Fingertip Formulary, and internal PA data show access reality. High potential means nothing if patient coverage creates barriers. Access-adjusted targeting factors formulary status, PA denial rates, and out-of-pocket costs into prioritization.
Digital Engagement
Email opens, webinar attendance, website visits, and portal activity reveal engagement patterns field data misses. An HCP attending competitor webinars signals interest—even without increased prescribing yet.
The Integration Challenge
The data exists but lives in five systems with different identifiers and update frequencies. Modern targeting platforms resolve identities automatically, creating unified HCP profiles combining all categories into a single, current view.
Tellius connects through pre-built connectors, handles identity resolution automatically, and maintains a pharma-native semantic layer understanding TRx, NBRx, deciles, formulary status, and territory structures natively.
How to Evaluate AI HCP Targeting Platforms
Not every platform claiming "AI-powered targeting" delivers the same capabilities. Here's what separates marketing claims from operational reality.
Essential Capabilities Checklist
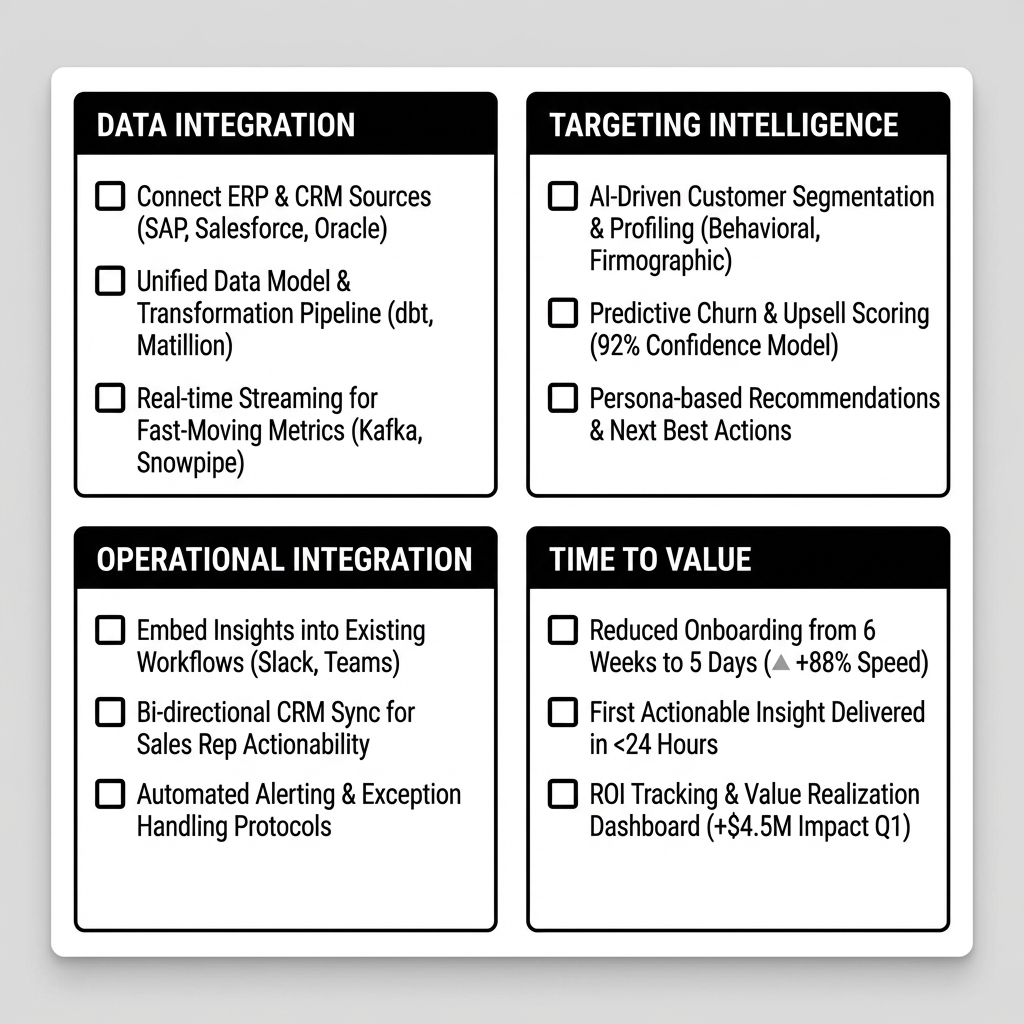
Questions to Ask Vendors
- "Show me a real HCP profile with all data sources unified. How current is the engagement data?" If they can't demo with actual data, they're showing slideware.
- "How do you handle HCP identity resolution when IQVIA and Veeva have different records?" If the answer involves "manual matching," dig deeper.
- "What happens to my target list when a major payer changes formulary status?" Static platforms require manual intervention. Agentic platforms adjust automatically.
- "Can you show me the drivers behind an HCP's score?" Explainability builds field trust.
- "How do I measure whether AI targeting improved prescribing vs. status quo?" Impact attribution separates sophisticated platforms from reporting tools.
AI-Powered HCP Targeting with Tellius
Tellius is an AI analytics platform with a 24/7 AI Analyst purpose-built for pharma commercial operations. The platform approaches targeting as one component of unified prescriber intelligence, not a standalone point solution creating another data silo.
Unified Prescriber Intelligence
Tellius connects directly to IQVIA and Symphony for prescriptions, Veeva and Salesforce for CRM, MMIT and Fingertip Formulary for payer data, plus internal systems. The platform resolves HCP identities automatically—"15 calls" in CRM means 15 calls everywhere.
When an HCP shows declining prescription volume, you know immediately whether it's an access problem (payer added PA), execution problem (territory vacancy), or competitive problem (competitor gained share). Without unified data, you're guessing.
Pharma-Native Semantic Layer
Tellius understands TRx, NBRx, deciles, SOB, formulary status, PA requirements, and territory structures natively. This isn't generic BI with a pharma skin—the semantic layer encodes pharmaceutical commercial logic from the ground up, forming the foundation of unified prescriber intelligence.
Brand managers ask questions in plain English: "Show me HCPs in Region 3 with declining NBRx but favorable payer access." Answers return in seconds, not analyst tickets.
Agentic Targeting Intelligence
AI agents don't score HCPs once and wait for quarterly refresh. They monitor continuously, detect changes, and alert teams before problems become surprises.
When a high-value target stops responding, when a payer adds restrictions, when a competitor gains ground—AI agents surface it with root cause analysis and recommended next steps. This is the difference between reactive analytics and proactive intelligence.
Access-Adjusted Prioritization
High-potential HCPs with bad payer coverage are low-value targets. Tellius factors formulary status, PA denial rates, and patient out-of-pocket costs into scores so reps focus where prescriptions can actually convert.
Deployment: 8-12 weeks to first value. Works alongside existing Veeva, Salesforce, and analytics infrastructure.

What AI-Powered HCP Targeting Delivers
A biotech launching a rare cancer therapy described their challenge as "a needle in a haystack." Traditional targeting based on historical oncology prescribing missed physicians treating the specific patient population.
Using Tellius, the team joined internal and external prescriber datasets and trained an ML-based targeting model—without data scientists. The model identified non-target HCPs with high propensity: physicians with the right patient mix and favorable access who'd been invisible below historical decile thresholds. Within six months: 30% increase in starts, multimillion-dollar revenue impact. (For a similar transformation story, see how Novo Nordisk moved from 2D to 3D commercial operations with AI analytics.)
Frequently Asked Questions About HCP Targeting for Pharma
Part 1: Evaluating Platforms
What is AI-powered HCP targeting for pharma?
AI-powered HCP targeting uses machine learning to identify, score, and prioritize healthcare professionals most likely to prescribe or increase prescribing—building what leading commercial teams call unified prescriber intelligence. Traditional decile-based targeting ranks HCPs by historical volume alone. AI-powered platforms combine prescription data, CRM activity, digital engagement, claims data, and payer access to predict future potential. For commercial teams, this means finding high-potential HCPs before competitors, detecting disengagement 60-90 days earlier, and adjusting targets weekly instead of annually.
What should I look for in an HCP targeting platform for pharma?
Evaluate against five criteria: pharma-native data integration (IQVIA, Symphony, Veeva, payer sources without custom development), explainable scoring showing why an HCP is prioritized, access-adjusted targeting factoring formulary and PA rates, continuous monitoring alerting on market changes, and deployment in weeks not years. Tellius meets all five: pre-built connectors, transparent score drivers, payer-integrated prioritization, agentic monitoring, and 8-12 week deployment.
Should we build or buy an HCP targeting solution?
Building on Snowflake or Databricks offers flexibility but requires 6-12 months and dedicated ML engineering—HCP identity resolution, predictive models, CRM integration, and ongoing maintenance. Purpose-built platforms deploy in 8-12 weeks pre-configured for pharma. Build if you have unique requirements and internal ML capacity. Buy if you need results in one quarter and want resources focused on commercial execution.
How does Tellius compare to Veeva Align for HCP targeting?
Veeva Align handles territory alignment, call planning, and roster management—operational functions ensuring balanced workloads. Tellius adds predictive intelligence: identifying untapped potential, detecting early disengagement, adjusting priorities as access and competitive dynamics shift. Veeva Align answers "who is assigned?" Tellius answers "which assigned HCPs should this rep prioritize this week, and why?"
How does AI-powered HCP targeting compare to traditional decile-based targeting?
Decile-based targeting ranks HCPs by historical prescription volume—backward-looking and updated annually. AI-powered targeting combines multiple data sources to predict future potential, adjusting weekly. Deciles miss high-potential HCPs below volume thresholds; AI surfaces them by factoring payer access, patient mix, digital engagement, and competitive dynamics into scores that explain why an HCP deserves attention.
What data privacy considerations apply to AI-powered HCP targeting?
AI-powered targeting uses commercially available prescription data (IQVIA, Symphony), CRM activity, and payer data—not protected health information. Platforms should maintain HIPAA-compliant data handling, role-based access controls, and audit trails. Patient-level data (APLD) requires additional safeguards. Evaluate vendors on data governance practices, not just analytical capabilities.
Part 2: Implementation
How long does it take to deploy AI-powered targeting?
Purpose-built platforms deploy in 8-12 weeks. Weeks 1-3: data connection and identity resolution. Weeks 4-6: model configuration and validation. Weeks 7-10: CRM integration. Weeks 10-12: pilot rollout and tuning. Compare to custom builds (6-12 months) or legacy implementations (12-18 months).
How does AI-powered targeting change the rep's job?
Reps shift from working stale lists with no context to receiving weekly priorities based on current intelligence. Instead of guessing which HCPs to prioritize, they get pre-call briefs with relevant context and alerts on engagement signals. The job evolves from "hit call targets on a static list" to "engage the right HCPs with the right message at the right time." (See AI analytics for pharma field sales for how this plays out in practice.)
Part 3: Strategy and ROI
Can AI targeting replace deciles entirely?
Most organizations combine approaches. Deciles ensure proven high-volume HCPs receive consistent coverage. Predictive scoring adds forward-looking signals: emerging writers, access-advantaged opportunities, disengagement risks. Best practice uses deciles as one input alongside dynamic scoring, prioritizing HCPs with both track record and future potential.
What's the ROI timeline for AI-powered targeting?
Measurable impact typically within 6-9 months. First wins: eliminating wasted effort on low-value targets and reallocating calls to higher-potential HCPs. Larger wins: finding hidden opportunities—HCPs with favorable access and untapped potential who weren't on anyone's radar. One biotech saw 30% increase in starts within six months. ROI compounds as targeting accuracy improves over time.
How does Tellius pricing work?
Tellius pricing scales with data volume and user count. Most implementations start with a pilot—one brand, one region—to prove value before enterprise commitment. Contact Tellius directly for specific pricing based on your data footprint and deployment scope.
Can we run a pilot before full deployment?
Yes, and Tellius recommends it. A typical pilot runs 8-12 weeks covering one brand or region, validating data integration, model accuracy, field adoption, and measurable impact. Pilots surface change management requirements and integration details. Most enterprise deployments start as successful pilots that expanded.
Stop Chasing Last Year's Scripts
Your competitors are still working from static decile lists outdated the day they were published. Leading pharma commercial teams have moved to unified prescriber intelligence—AI-powered targeting that finds high-potential HCPs 90 days earlier, detects prescriber churn before it hits revenue, and adjusts dynamically as markets shift.
The question isn't whether AI targeting works—that's proven across therapeutic areas and company sizes. The question is whether your organization will build unified prescriber intelligence or cede the opportunity to faster-moving competitors.
Get release updates delivered straight to your inbox.
No spam—we hate it as much as you do!


.webp)
Best AI Platforms for Pharma Commercial Analytics in 2026: 11 Platforms Compared
This guide compares the 11 best AI platforms for pharma commercial analytics in 2026, evaluating how each supports brand performance, market access, patient analytics, field force effectiveness, incentive compensation, and omnichannel engagement. It highlights a key shift in the market: traditional BI and SFE tools focus on reporting what happened, while newer AI platforms differentiate by investigating why performance changed. The post breaks down core capabilities like root cause analysis, data integration, governance, and agentic workflows—helping pharma teams identify which platforms can deliver faster, more actionable insights across commercial operations.