AI for Next Best Action in Pharma: Why Most Programs Fail (And What Actually Works)
.webp)
.png)
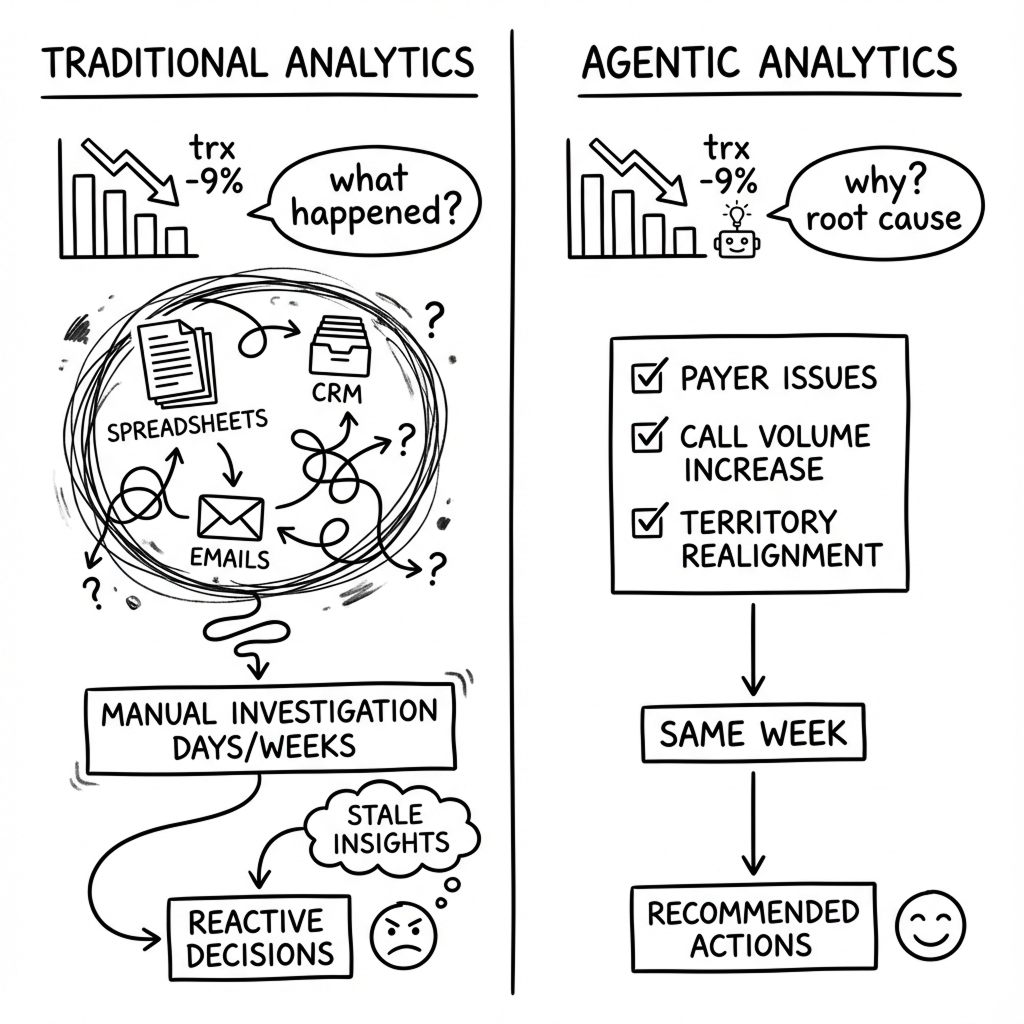
Your regional dashboard says TRx is down 9% versus plan in the West. Two territories are red. By the time you’re on the Monday call, you’ve already heard three competing explanations:
- “Territory realignment messed everything up.”
- “Access just tightened at a big payer.”
- “Reps are slacking on calls.”
So you do what you always do. Pull up CRM. Export some claims data to Excel. Dig through email threads about formulary updates. Three hours later, the only thing you know for sure is that whatever happened started weeks ago—and you're no closer to fixing it.
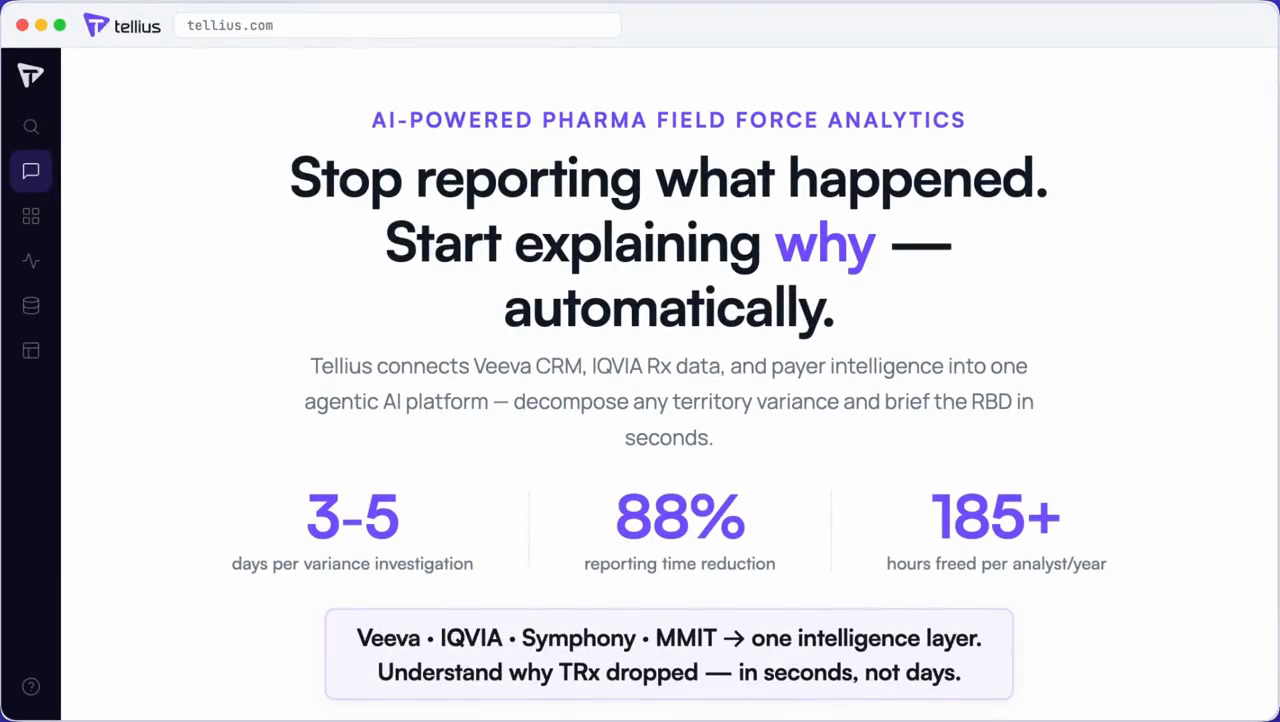
Sound familiar? It should. This is field force analytics at most pharma companies right now. Dashboards that tell you what happened. Rarely why. Almost never what to do about it.
I've spent the last few years watching pharma commercial teams try to fix this with AI. Some are getting real results with AI-powered field force analytics. Most are not. This post is about the difference—and what actually works for sales force effectiveness in pharma.
The hype versus reality gap
IQVIA states that over 80% of major pharma companies have deployed some form of next-best-action in the field. McKinsey says AI could create $18–30 billion in annual value for pharma commercial functions.
Sounds great. Except if you spend ten minutes on practitioner channels, you hear a different story. Reps talk about "fire drills," quota chaos, and target list whiplash. One analytics leader put it bluntly:

The problem isn't that companies aren't trying AI. The problem is they're bolting AI onto broken data foundations—so "next best action" becomes "next best guess."
The teams seeing results tend to use agentic analytics platforms rather than standalone NBA models—systems that can investigate, explain, and adapt, not just score and rank.
Over the past decade, the field environment has become brutally constrained. In-person access to HCPs dropped to roughly 40–45% at its low point and has only partially recovered, with many “accessible” physicians limiting how many companies they see. At the same time, interaction time has shrunk to minutes: often less than the time it took you to read this paragraph. Inside that narrow window, reps are expected to hit aggressive reach and frequency goals, stay compliant with complex promo rules, and tailor messaging to each HCP's history.
From Pilots to Production: What's Actually Working
Strip away vendor hype and a clear pattern emerges from teams getting real impact.
A large biotech deployed ML-driven next-best-action for its specialty field team. Instead of reps manually sifting decile lists, the system suggested specific HCPs with reasons: "Dr. K has 12 new patients with condition X and hasn't initiated therapy; similar HCPs in your territory have started prescribing."
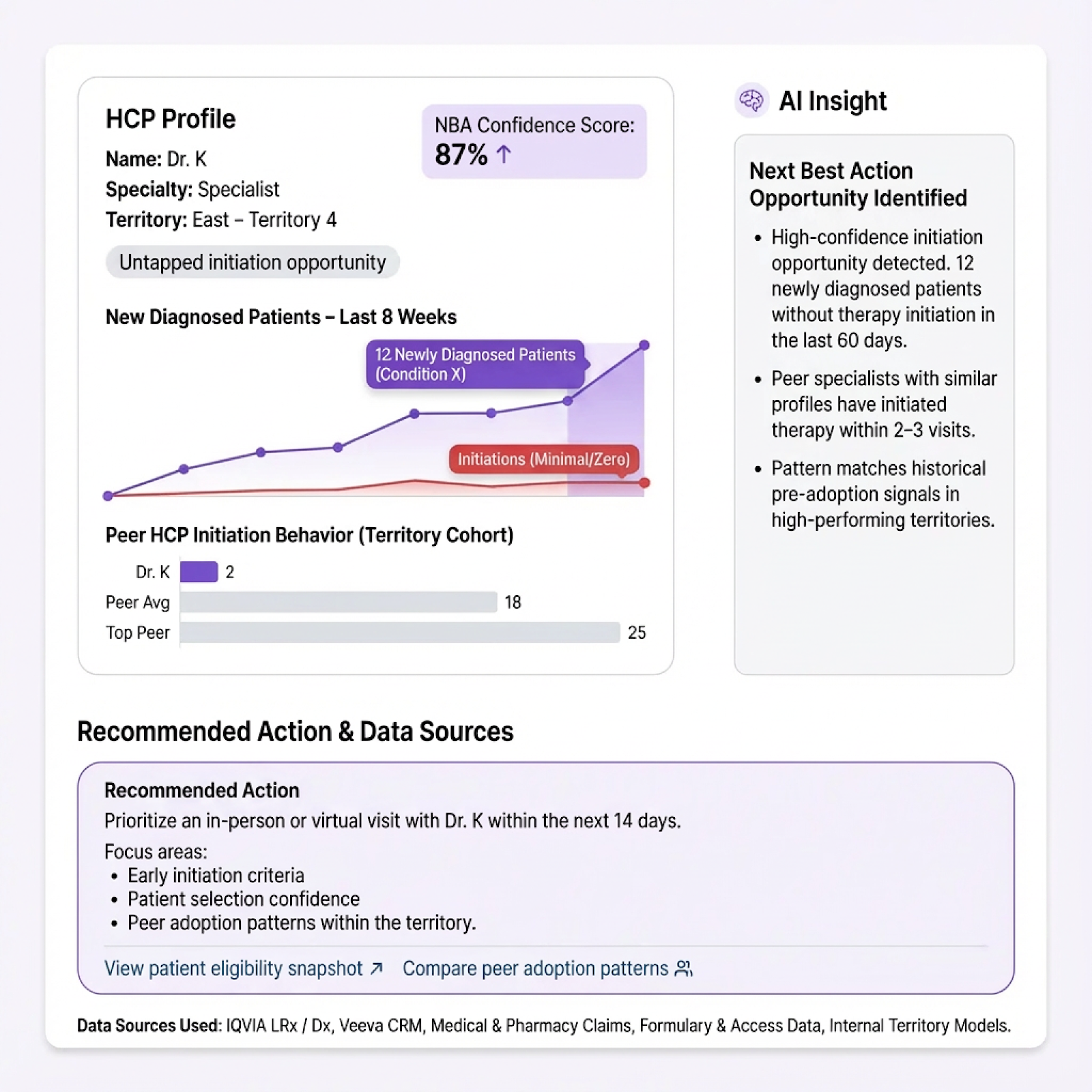
When reps followed the system more than half the time, brand leads saw double-digit uptick in new-to-brand Rx in pilot regions. The key: the data foundation and explanations were good enough that reps trusted the guidance.
At the 2025 annual PMSA conference and other industry forums, successful teams share common traits:
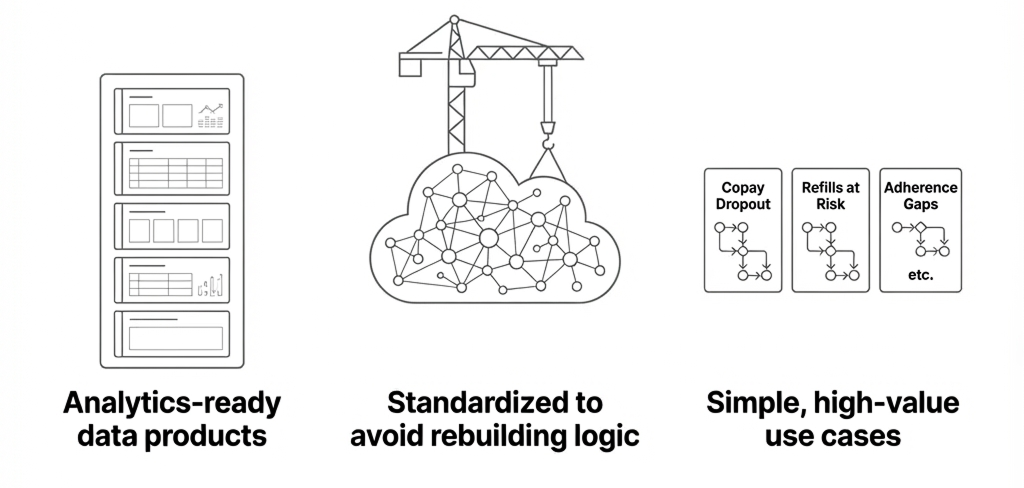
- They build "analytics-ready data products"—standardized, documented tables designed for AI workflows
- They standardize on cloud data warehouses plus semantic modeling to avoid rebuilding logic for every new brand or vendor
- They start with simple, high-value use cases (copay dropout, refills at risk) before expanding scope
Teams getting impact treat data architecture and explainability as first-class citizens.
Key takeaway: Teams that succeed with NBA treat data architecture and explainability as non-negotiable—not "phase two."
The tech that actually matters
I'll keep this as short as I can, but you can't skip the architecture piece—it's why most AI projects fail. The key is connecting real-world data (claims, CRM, access) with AI that actually understands pharma commercial operations.
1. Semantic Layer: Teaching AI Your Business
Most LLMs looking at raw database tables see column names like tbl_trx_agg and hcp_id_2. They don't know what NBRx means, how you calculate reach, or what a formulary tier change implies.
A semantic layer fixes that by encoding three things:
- Metric definitions: TRx, NBRx, reach, frequency, call success—exact formulas, not tribal knowledge
- Entity relationships: HCPs to locations, locations to health systems, patients to plans, reps to territories
- Business logic: What a tier change means for prescribing, what counts as sufficient reach, how to adjust for payer mix
One study found that giving an LLM proper business context took accuracy from single digits to nearly 80% on complex questions. That's the difference between useful and useless.
2. Identity Resolution: Killing the Ghost HCP Problem
The same cardiologist shows up as "John Smith MD" in CRM, "J.A. Smith" in claims, and "Jonathan Smith" in your digital data—with two different NPIs across vendors.
If you can't link them reliably, everything downstream breaks:
- Your propensity models are wrong
- Your territory rollups are wrong
- Your attribution of rep impact versus access impact is wrong
I know this sounds like plumbing. It is. But every "why is this HCP's behavior changing?" question depends on it being solved once, properly.
3. Agentic Analytics: Beyond "Chat with Your Data"
Most conversational analytics demos stop at "I asked a question and got a chart." That's not enough for field force decisions.
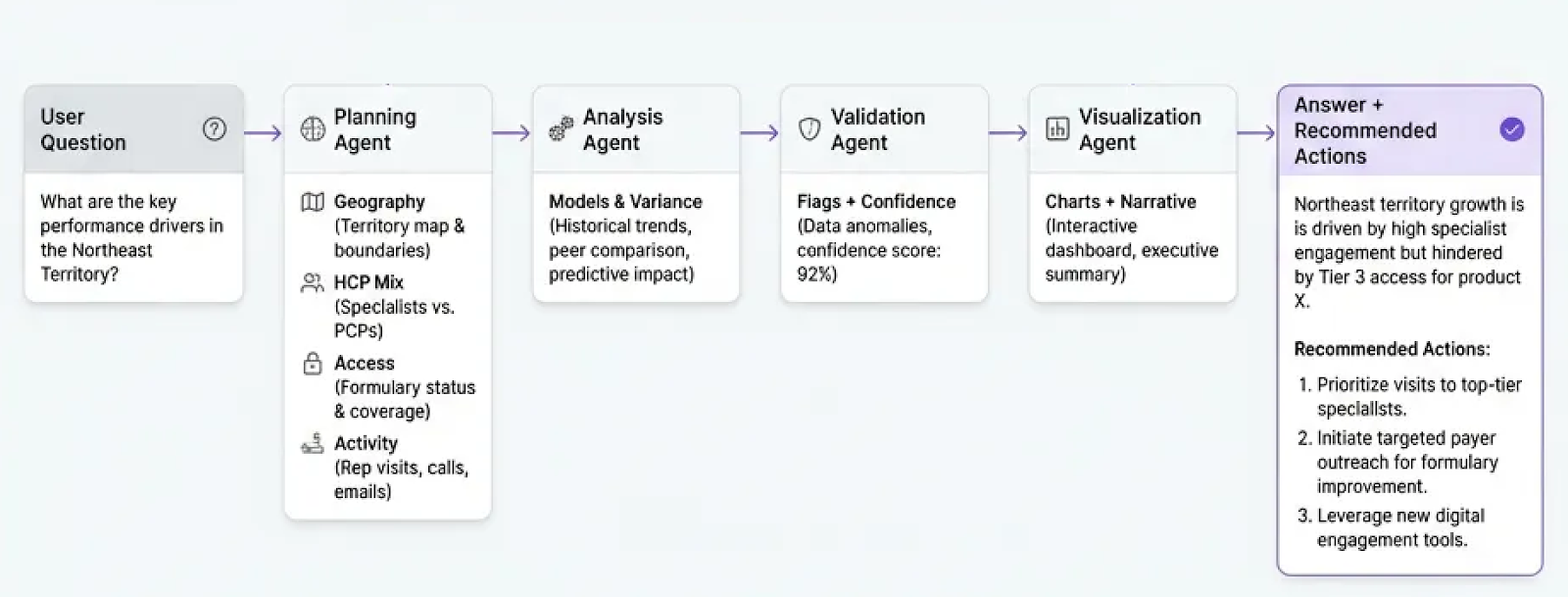
The real shift is agentic analytics—systems that don't just answer questions but decide which questions to ask and then do the work. A strong architecture includes:
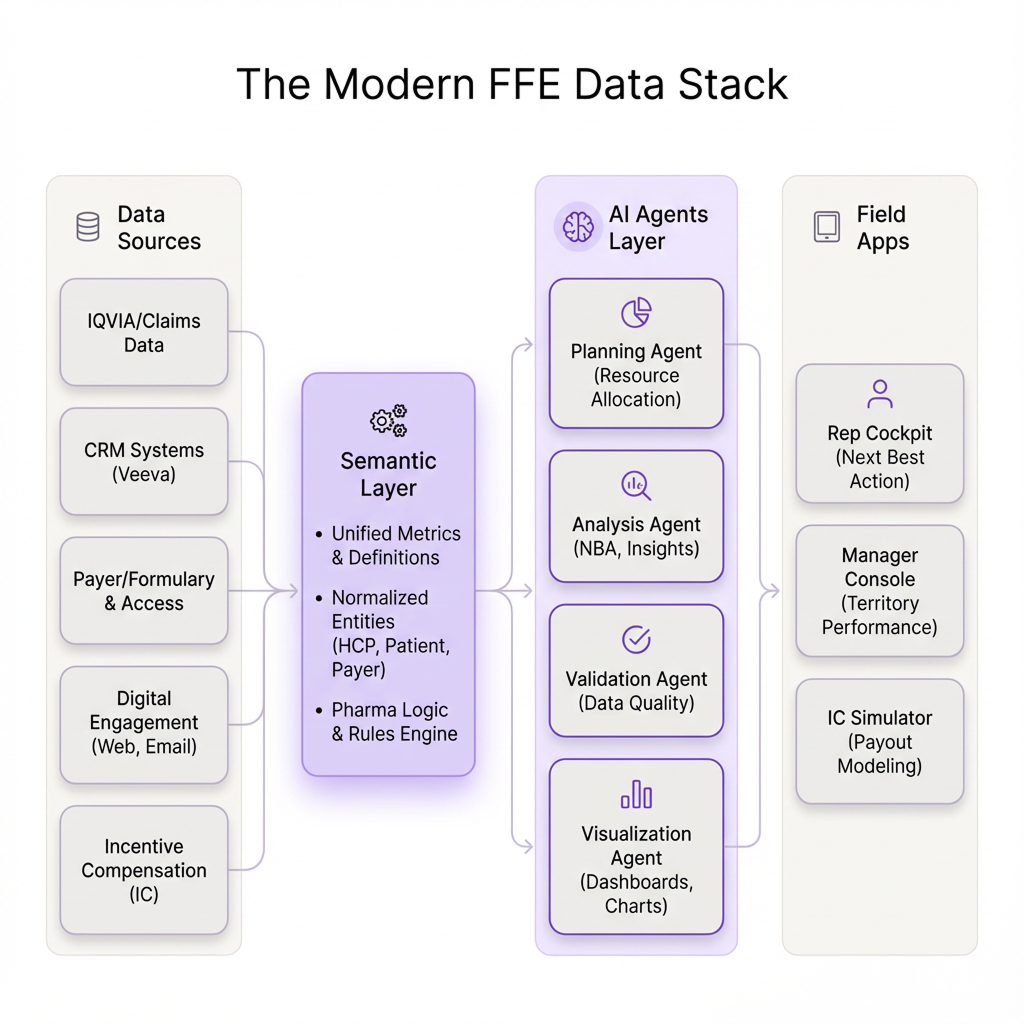
- Planning agent: Figures out what analyses are needed to answer "Why did TRx drop in the Southwest?"
- Analysis agent: Runs variance decomposition, cohort analysis, anomaly detection
- Validation agent: Checks for data gaps, statistical noise, conflicting signals—flags high-confidence versus speculative findings
- Visualization agent: Chooses the right charts and narratives to explain what's happening
The key difference: reasoning is traceable. A field leader can see how the system decomposed the problem, what data it used, and how confident it is in each driver. That's what converts AI from toy to trusted analyst.
4. Right-Time Processing
Not every use case needs millisecond streaming. Claims data still updates weekly for most brands. What you actually need:
- Daily or weekly refresh of claims and CRM data
- Near-real-time signals from digital engagement and access updates
- Automated re-analysis when new data lands
When the new week's claims hit, agents should automatically recompute territory progress, flag anomalies, attribute likely drivers, and generate briefs. That's "real-time enough" to change behavior this week, not next quarter.
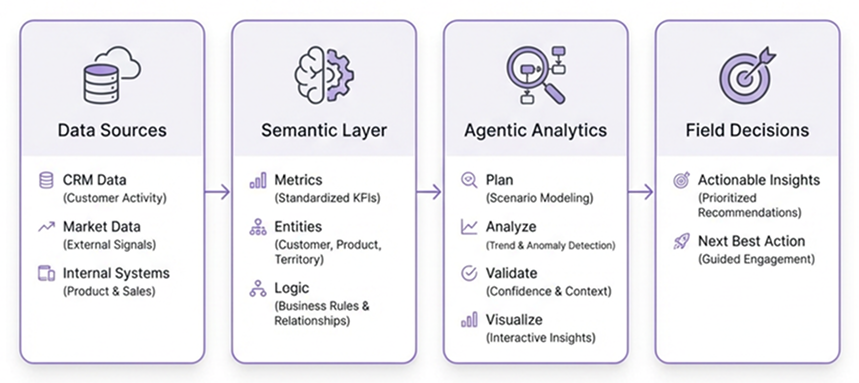
Key takeaway: The modern FFE stack flows from Data → Semantic Layer → Agentic Analytics → Decisions. Skip any layer and the whole thing breaks.
Four use cases where AI is moving numbers in pharma sales
Let me get specific about where AI for field force effectiveness is changing pharma commercial operations today.
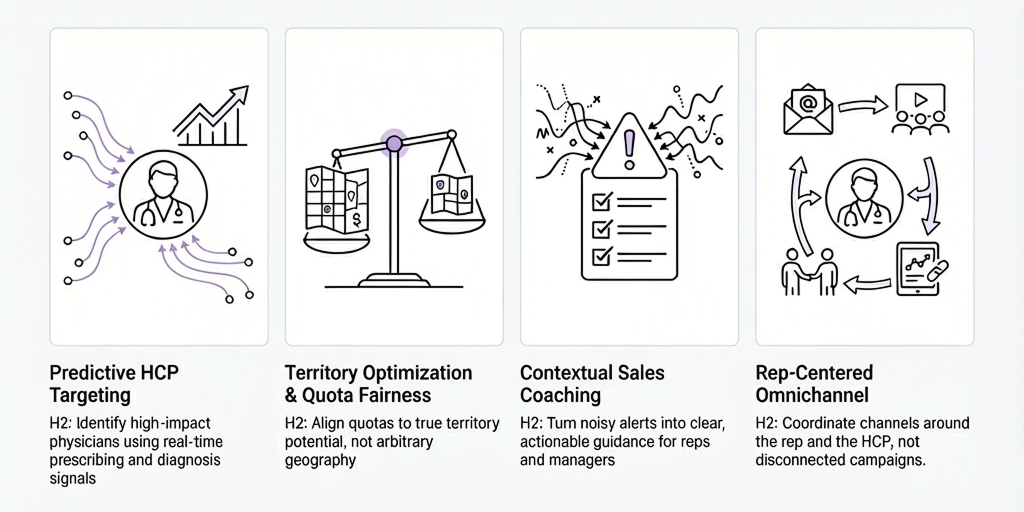
1. Predictive HCP Targeting: Finding the Doctors Who Actually Matter
Every sales org claims they "prioritize high-value HCPs." In reality, a lot of targeting still runs on last year's deciles, rep gut feel, and lists that update twice a year. You end up with reps chasing retired physicians and no-see offices.
The Pareto rule is brutal in pharma sales: 20% of HCPs drive 80% of prescriptions. The job of modern pharma commercial analytics is making that visible and keeping it current:
- Pull in claims trends, new diagnosis signals, referral patterns, digital engagement
- Score HCPs on propensity to write and responsiveness to promotion
- Refresh scores as new data arrives
- Explain the reasoning: "Her panel grew 25% in your condition, she matches high-writing peers, she hasn't seen you in 90 days"
The rep still decides. But they're not flying blind.
2. Territory Optimization & Quota Fairness: Ending "Geography Is Destiny"
This one's personal for reps—and critical for pharma sales force effectiveness. Nothing kills morale faster than believing the game is rigged.
"My territory is mostly Medicaid with brutal prior auths. Why am I ranked against people in commercially rich metros?"
When quota setting ignores payer mix and access friction, you create unwinnable territories where great reps burn out and gift territories where mediocre reps coast. Research backs this up—employees who believe their goals are achievable are significantly more engaged. In sales, "engaged" means "still trying in week 10."
With the right data architecture:
- Compute territory potential that accounts for payer mix, prevalence, and access friction
- Simulate different territory boundaries and quota distributions
- Flag territories where performance is off relative to potential, not a flat national target
Performance reviews shift from "you missed quota" to "you captured 85% of realistic potential—here's what's blocking the rest." That's a coaching conversation, not an interrogation.
3. Coaching that doesn't create alert fatigue
Every company that tries "real-time alerts" ends up in the same place. Week one, everyone's excited. Week four, nobody reads them.
Why? The alerts are noisy, lack context, and offer no next step.
Instead of: "Territory Southwest down 10% vs. last month."
You want: "Southwest down 10% vs. plan. 60% of the gap comes from three high-potential HCPs whose NBRx dropped. Their patients' out-of-pocket costs just increased due to a plan change. None have been detailed on your access support program.
Recommended actions: Prioritize visits to these three HCPs this week. Lead with access messaging. Sync with market access on co-pay adjustments."
Now the manager knows where to coach and the rep knows what to do. That's the difference.
4. Making omnichannel work around the rep
Here's the current state at most companies: marketing blasts emails with no idea what the rep just said in-office. Reps walk into calls not knowing the HCP attended a webinar yesterday. The HCP gets the same message three times from three channels and tunes everyone out.
HCPs aren't frustrated by too much communication. They're frustrated by irrelevant, redundant communication.
With proper data integration, agents can:
- Build per-HCP engagement timelines across channels
- Learn which sequences actually move prescribing behavior
- Suggest next-best-channel, not just next-best-call
So the recommendation isn't just "visit Dr. Nguyen." It's: "Dr. Nguyen engaged with your safety email and attended last week's webinar—follow up on that within seven days for maximum impact."
Key takeaway: The four use cases that actually move numbers—HCP targeting, territory fairness, real-time coaching, and omnichannel orchestration—all depend on the same foundation: connected data, semantic understanding, and explainable AI.
Implementation reality (a.k.a. the boring stuff nobody wants to talk about)
The tech is ahead of most organizations. Implementation is where things get hard.
Governance is an afterthought
About three-quarters of pharma companies are using AI, but barely half have formal policies around it. Agents are making recommendations, and nobody's documented who's accountable when they're wrong.
At minimum you need:
- Clear ownership: Every major agent has a named business owner
- Documented playbooks: When can an agent act autonomously versus only recommend?
- Auditability: You can reconstruct why an agent made any recommendation
Simple rule: agents propose, humans decide. Especially when comp or compliance is involved.
Change management is underrated
Drop an AI copilot into a field org that's been burned by bad targeting and quota chaos, and you won't get adoption. You'll get eye rolls.
You have to earn trust:
- Start with use cases obviously in the rep's interest—"here's where you're losing scripts to access barriers" lands better than "here's how to do more calls"
- Show the system being right, publicly, in pipeline meetings
- Let reps flag bad recommendations and make it visible that feedback matters
If the first three experiences miss the mark, reps quietly go back to Excel—and adoption quietly stalls.
Crawl → Walk → Run
If your instinct is to immediately draw a "Field AI operating model 2030" slide, resist it.
A more realistic FFE roadmap looks like:
1. Crawl – Fix the foundations
- Build the semantic layer for FFE metrics and entities
- Clean up HCP identity and territory definitions
- Connect CRM + claims + access as a minimally viable unified view
2. Walk – Deploy one meaningful agentic workflow
- Pick a high-leverage, low-politics problem (e.g., territory performance diagnosis or early NBRx slippage detection)
- Let agents run the analysis but keep humans firmly in control of decisions
- Measure time saved and quality of decisions vs. your previous Excel-and-slide routine
3. Run – Expand to adjacent workflows
- Add predictive HCP targeting, quota fairness, omnichannel suggestions
- Tighten governance and monitoring as complexity grows
- Eventually let some low-risk actions be automated end-to-end (e.g., updating call plans or sending internal alerts)
You earn the right to "autonomous agents everywhere" by proving you can safely automate one FFE loop first.
Where Tellius Kaiya fits
Everything I've described requires three things working together:
- A semantic layer that understands pharma commercial—so you're not defining TRx from scratch for every project
- An agentic analytics engine that plans analyses, runs the work, validates results, and explains what it found
- A conversational interface where field leaders can ask real questions and get real answers—not just prettier charts
.png)
That's what we built Kaiya to do. It sits on your data and actually knows your business. It uses specialized agents to handle complex questions without hallucinating. It connects to the tools reps and managers already use.
When these pieces come together, Monday morning looks different:
- Reps spend time on the right HCPs
- Territories and quotas feel fair enough to fight for
- Managers know why performance moved, not just that it moved
- Your field data exhaust becomes a strategic asset
The bottom line
The technology for AI-powered pharma sales analytics is ready. The architecture patterns are proven. The constraint now is organizational: will commercial leaders invest in data foundations, set guardrails, and build with reps instead of just deploying at them?
The companies that get field force effectiveness right won't just eke out a few extra TRx points. They'll change what a good pharma sales team looks like—more focused, more effective, supported by systems that finally close the gap between "what happened" and "what to do next."
Get release updates delivered straight to your inbox.
No spam—we hate it as much as you do!

Next best action is an AI-driven approach that recommends which HCPs a rep should prioritize, what message to deliver, and through which channel—based on real-time data rather than static call lists. The goal is to move from generic targeting to personalized, timely recommendations that actually influence prescribing behavior.
The best NBA platform is the one that solves pharma’s unique data problem first. Look for a system with a pre-built semantic layer for commercial metrics (TRx, NBRx, reach, frequency), automated HCP identity resolution across CRM and claims, and agentic analytics that investigates root causes rather than just answering queries. Most importantly, the platform needs to explain its recommendations in language reps trust. Tellius Kaiya was built specifically for this: combining pharma-native data modeling, multi-agent reasoning, and conversational interfaces that field teams actually use.
The most common reason: NBA models get bolted onto broken data foundations. When HCP identity is fragmented, metrics are inconsistent, and data lives in silos, even sophisticated AI produces "next best guesses." The second killer is lack of explainability—reps don't trust black-box recommendations, so they ignore them.
At minimum: claims/Rx data, CRM activity, and formulary/access information. For more advanced use cases, you'll also need digital engagement data, patient-level insights (where permissible), and payer mix by territory. The key isn't just having the data—it's having it linked, cleaned, and semantically modeled so AI can actually use it.
Traditional targeting relies on static deciles and annual list updates. AI-powered predictive HCP targeting pulls in real-time signals—new patient diagnoses, prescribing trend changes, referral patterns, digital engagement—and continuously re-scores HCPs on propensity and responsiveness. More importantly, it explains why an HCP is prioritized, which drives rep trust and adoption.
Traditional BI answers the question you asked with a chart. Agentic analytics investigates—it breaks your question into sub-analyses, runs the appropriate methods, validates the results, and explains what it found. Instead of "here's TRx by territory," you get "TRx dropped 10% in Southwest, driven primarily by three HCPs whose patients faced access barriers after a payer change—here's what to do about it."
Skip vanity metrics like "dashboard logins" or "AI adoption rate." Focus on outcomes: Did rep behavior change? Did new-to-brand Rx increase in pilot regions? Did time-to-insight shrink? The biotech example in this post saw double-digit NBRx lift when reps followed AI recommendations more than half the time—that's the kind of signal that matters.
It depends on your data foundation. If your semantic layer, HCP identity, and core data connections are solid, you can deploy a meaningful agentic workflow in 8–12 weeks. If you're starting from fragmented data and inconsistent definitions, expect 3–6 months of foundation work before AI adds real value. The "crawl → walk → run" approach helps teams show results faster while building toward scale.
Traditional BI in pharma is reactive—dashboards that show what happened last month or last quarter. Modern pharma commercial analytics powered by AI is proactive: it detects anomalies, diagnoses root causes, and recommends actions before the quarter is lost. The shift is from "reporting on the past" to "guiding the next best action."
.png)
Best AI Platforms for Pharma Field Force Effectiveness and Sales Analytics in 2026: 10 Platforms Compared (Plus 3 General BI Alternatives)
A 2026 comparison of 10 AI platforms for pharma Field Force Effectiveness, focused on what actually separates “agentic” FFE analytics from dashboards: automated deep insights (root cause), proactive monitoring, governed Q&A, pharma data integrations, and workflow orchestration—plus clear “best for” recommendations by use case and team maturity.